
Mouth-to-mouth resuscitation, a form of artificial ventilation, is the act of assisting or stimulating respiration in which a rescuer presses their mouth against that of the victim and blows air into the person's lungs. Artificial respiration takes many forms, but generally entails providing air for a person who is not breathing or is not making sufficient respiratory effort on their own. It is used on a patient with a beating heart or as part of cardiopulmonary resuscitation (CPR) to achieve the internal respiration.

A ventilator is a type of breathing apparatus, a class of medical technology that provides mechanical ventilation by moving breathable air into and out of the lungs, to deliver breaths to a patient who is physically unable to breathe, or breathing insufficiently. Ventilators may be computerized microprocessor-controlled machines, but patients can also be ventilated with a simple, hand-operated bag valve mask. Ventilators are chiefly used in intensive-care medicine, home care, and emergency medicine and in anesthesiology.

Mechanical ventilation or assisted ventilation is the medical term for using a machine called a ventilator to fully or partially provide artificial ventilation. Mechanical ventilation helps move air into and out of the lungs, with the main goal of helping the delivery of oxygen and removal of carbon dioxide. Mechanical ventilation is used for many reasons, including to protect the airway due to mechanical or neurologic cause, to ensure adequate oxygenation, or to remove excess carbon dioxide from the lungs. Various healthcare providers are involved with the use of mechanical ventilation and people who require ventilators are typically monitored in an intensive care unit.

Positive airway pressure (PAP) is a mode of respiratory ventilation used in the treatment of sleep apnea. PAP ventilation is also commonly used for those who are critically ill in hospital with respiratory failure, in newborn infants (neonates), and for the prevention and treatment of atelectasis in patients with difficulty taking deep breaths. In these patients, PAP ventilation can prevent the need for tracheal intubation, or allow earlier extubation. Sometimes patients with neuromuscular diseases use this variety of ventilation as well. CPAP is an acronym for "continuous positive airway pressure", which was developed by Dr. George Gregory and colleagues in the neonatal intensive care unit at the University of California, San Francisco. A variation of the PAP system was developed by Professor Colin Sullivan at Royal Prince Alfred Hospital in Sydney, Australia, in 1981.

An anaesthetic machine or anesthesia machine is a medical device used to generate and mix a fresh gas flow of medical gases and inhalational anaesthetic agents for the purpose of inducing and maintaining anaesthesia.
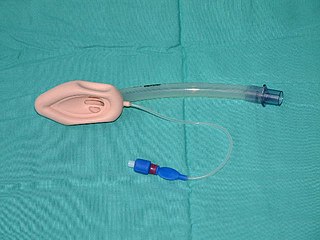
A laryngeal mask airway (LMA), also known as laryngeal mask, is a medical device that keeps a patient's airway open during anaesthesia or while they are unconscious. It is a type of supraglottic airway device. They are most commonly used by anaesthetists to channel oxygen or inhalational anaesthetic to the lungs during surgery and in the pre-hospital setting for unconscious patients.

Airway management includes a set of maneuvers and medical procedures performed to prevent and relieve airway obstruction. This ensures an open pathway for gas exchange between a patient's lungs and the atmosphere. This is accomplished by either clearing a previously obstructed airway; or by preventing airway obstruction in cases such as anaphylaxis, the obtunded patient, or medical sedation. Airway obstruction can be caused by the tongue, foreign objects, the tissues of the airway itself, and bodily fluids such as blood and gastric contents (aspiration).

Respiratory arrest is a serious medical condition caused by apnea or respiratory dysfunction severe enough that it will not sustain the body. Prolonged apnea refers to a patient who has stopped breathing for a long period of time. If the heart muscle contraction is intact, the condition is known as respiratory arrest. An abrupt stop of pulmonary gas exchange lasting for more than five minutes may permanently damage vital organs, especially the brain. Lack of oxygen to the brain causes loss of consciousness. Brain injury is likely if respiratory arrest goes untreated for more than three minutes, and death is almost certain if more than five minutes.

Artificial ventilation is a means of assisting or stimulating respiration, a metabolic process referring to the overall exchange of gases in the body by pulmonary ventilation, external respiration, and internal respiration. It may take the form of manually providing air for a person who is not breathing or is not making sufficient respiratory effort, or it may be mechanical ventilation involving the use of a mechanical ventilator to move air in and out of the lungs when an individual is unable to breathe on their own, for example during surgery with general anesthesia or when an individual is in a coma or trauma.
A resuscitator is a device using positive pressure to inflate the lungs of an unconscious person who is not breathing, in order to keep them oxygenated and alive. There are three basic types: a manual version consisting of a mask and a large hand-squeezed plastic bulb using ambient air, or with supplemental oxygen from a high-pressure tank. The second type is the expired air or breath powered resuscitator. The third type is an oxygen powered resuscitator. These are driven by pressurized gas delivered by a regulator, and can either be automatic or manually controlled. The most popular type of gas powered resuscitator are time cycled, volume constant ventilators. In the early days of pre-hospital emergency services, pressure cycled devices like the Pulmotor were popular but yielded less than satisfactory results. Most modern resuscitators are designed to allow the patient to breathe on his own should he recover the ability to do so. All resuscitation devices should be able to deliver more than 85% oxygen when a gas source is available.

A breathing apparatus or breathing set is equipment which allows a person to breathe in a hostile environment where breathing would otherwise be impossible, difficult, harmful, or hazardous, or assists a person to breathe. A respirator, medical ventilator, or resuscitator may also be considered to be breathing apparatus. Equipment that supplies or recycles breathing gas other than ambient air in a space used by several people is usually referred to as being part of a life-support system, and a life-support system for one person may include breathing apparatus, when the breathing gas is specifically supplied to the user rather than to the enclosure in which the user is the occupant.
High-frequency ventilation is a type of mechanical ventilation which utilizes a respiratory rate greater than four times the normal value and very small tidal volumes. High frequency ventilation is thought to reduce ventilator-associated lung injury (VALI), especially in the context of ARDS and acute lung injury. This is commonly referred to as lung protective ventilation. There are different types of high-frequency ventilation. Each type has its own unique advantages and disadvantages. The types of HFV are characterized by the delivery system and the type of exhalation phase.

A pocket mask, pocket face mask, or CPR mask is a device used to safely deliver rescue breaths during a cardiac arrest or respiratory arrest. The specific term "Pocket Mask" is the trademarked name for the product manufactured by Laerdal Medical AS. It is not to be confused with a bag valve mask (BVM).

A non-rebreather mask is a device used in medicine to assist in the delivery of oxygen therapy. A NRB requires that the patient can breathe unassisted, but unlike a low-flow nasal cannula, the NRB allows for the delivery of higher concentrations of oxygen. An ideal non-rebreather mask does not permit air from the surrounding environment to be inhaled, hence an event of a source gas failure is life-threatening.
A flow-restricted, oxygen-powered ventilation device (FROPVD), also referred to as a manually triggered ventilation device (MTV), is used to assist ventilation in apneic or hypoventilating patients, although these devices can also be used to provide supplemental oxygen to breathing patients. It can be used on patients with spontaneous breaths, as there is a valve that opens automatically on inspiration. When ventilating a patient with a (FROPVD) you must ensure an adequate, constant oxygen supply is available. Once the oxygen source is depleted, the device can no longer be used because it is driven completely by an oxygen source. The (FROPVD) has a peak flow rate of 100% oxygen at up to 40 liters per minute. To use the device, manually trigger it until chest rise is noted and then release. Wait five seconds before repeating. The device must have a pressure relief valve that opens at 60cm of water pressure to avoid over ventilation and trauma to the lungs. The (FROPVD) is contraindicated in adult patients with potential chest trauma and all children. Note: Proper training and considerable practice is required to correctly use the FROPVD devices.

An orinasal mask, oro-nasal mask or oral-nasal mask is a breathing mask that covers the mouth and the nose only. It may be a complete independent item, as an oxygen mask, or on some anaesthetic apparatuses, or it may be fitted as a component inside a fullface mask on underwater breathing apparatus, a gas mask or an industrial respirator to reduce the amount of dead space. It may be designed for its lower edge to seal on the front of the lower jaw or to go under the chin.
Modes of mechanical ventilation are one of the most important aspects of the usage of mechanical ventilation. The mode refers to the method of inspiratory support. In general, mode selection is based on clinician familiarity and institutional preferences, since there is a paucity of evidence indicating that the mode affects clinical outcome. The most frequently used forms of volume-limited mechanical ventilation are intermittent mandatory ventilation (IMV) and continuous mandatory ventilation (CMV). There have been substantial changes in the nomenclature of mechanical ventilation over the years, but more recently it has become standardized by many respirology and pulmonology groups. Writing a mode is most proper in all capital letters with a dash between the control variable and the strategy.

Neonatal resuscitation, also known as newborn resuscitation, is an emergency procedure focused on supporting approximately 10% of newborn children who do not readily begin breathing, putting them at risk of irreversible organ injury and death. Many of the infants who require this support to start breathing breath well on their own after assistance. Through positive airway pressure, and in severe cases chest compressions, medical personnel certified in neonatal resuscitation can often stimulate neonates to begin breathing on their own, with attendant normalization of heart rate.
A negative pressure ventilator (NPV) is a type of mechanical ventilator that stimulates an ill person's breathing by periodically applying negative air pressure to their body to expand and contract the chest cavity.
A breathing apparatus or breathing set is equipment which allows a person to breathe in a hostile environment where breathing would otherwise be impossible, difficult, harmful, or hazardous, or assists a person to breathe. A respirator, medical ventilator, or resuscitator may also be considered to be breathing apparatus. Equipment that supplies or recycles breathing gas other than ambient air in a space used by several people is usually referred to as being part of a life-support system, and a life-support system for one person may include breathing apparatus, when the breathing gas is specifically supplied to the user rather than to the enclosure in which the user is the occupant.


