Hearing loss is a partial or total inability to hear. Hearing loss may be present at birth or acquired at any time afterwards. Hearing loss may occur in one or both ears. In children, hearing problems can affect the ability to acquire spoken language, and in adults it can create difficulties with social interaction and at work. Hearing loss can be temporary or permanent. Hearing loss related to age usually affects both ears and is due to cochlear hair cell loss. In some people, particularly older people, hearing loss can result in loneliness.

A burn is an injury to skin, or other tissues, caused by heat, cold, electricity, chemicals, friction, or ultraviolet radiation. Most burns are due to heat from hot liquids, solids, or fire. Burns occur mainly in the home or the workplace. In the home, risks are associated with domestic kitchens, including stoves, flames, and hot liquids. In the workplace, risks are associated with fire and chemical and electric burns. Alcoholism and smoking are other risk factors. Burns can also occur as a result of self-harm or violence between people (assault).

An occupational injury is bodily damage resulting from working. The most common organs involved are the spine, hands, the head, lungs, eyes, skeleton, and skin. Occupational injuries can result from exposure to occupational hazards, such as temperature, noise, insect or animal bites, blood-borne pathogens, aerosols, hazardous chemicals, radiation, and occupational burnout.

Cardiovascular disease (CVD) is any disease involving the heart or blood vessels. CVDs constitute a class of diseases that includes: coronary artery diseases, heart failure, hypertensive heart disease, rheumatic heart disease, cardiomyopathy, arrhythmia, congenital heart disease, valvular heart disease, carditis, aortic aneurysms, peripheral artery disease, thromboembolic disease, and venous thrombosis.
An occupational disease or industrial disease is any chronic ailment that occurs as a result of work or occupational activity. It is an aspect of occupational safety and health. An occupational disease is typically identified when it is shown that it is more prevalent in a given body of workers than in the general population, or in other worker populations. The first such disease to be recognised, squamous-cell carcinoma of the scrotum, was identified in chimney sweep boys by Sir Percival Pott in 1775. Occupational hazards that are of a traumatic nature are not considered to be occupational diseases.

A hip fracture is a break that occurs in the upper part of the femur, at the femoral neck or (rarely) the femoral head. Symptoms may include pain around the hip, particularly with movement, and shortening of the leg. Usually the person cannot walk.

Paratyphoid fever, also known simply as paratyphoid, is a bacterial infection caused by one of three types of Salmonella enterica. Symptoms usually begin 6–30 days after exposure and are the same as those of typhoid fever. Often, a gradual onset of a high fever occurs over several days. Weakness, loss of appetite, and headaches also commonly occur. Some people develop a skin rash with rose-colored spots. Without treatment, symptoms may last weeks or months. Other people may carry the bacteria without being affected; however, they are still able to spread the disease to others. Typhoid and paratyphoid are of similar severity. Paratyphoid and typhoid fever are types of enteric fever.
Fall prevention includes any action taken to help reduce the number of accidental falls suffered by susceptible individuals, such as the elderly (idiopathic) and people with neurological or orthopedic indications.
The Global Burden of Disease Study (GBD) is a comprehensive regional and global research program of disease burden that assesses mortality and disability from major diseases, injuries, and risk factors. GBD is a collaboration of over 3600 researchers from 145 countries. Under principal investigator Christopher J.L. Murray, GBD is based in the Institute for Health Metrics and Evaluation (IHME) at the University of Washington and funded by the Bill and Melinda Gates Foundation.

A non-communicable disease (NCD) is a disease that is not transmissible directly from one person to another. NCDs include Parkinson's disease, autoimmune diseases, strokes, heart diseases, cancers, diabetes, chronic kidney disease, osteoarthritis, osteoporosis, Alzheimer's disease, cataracts, and others. NCDs may be chronic or acute. Most are non-infectious, although there are some non-communicable infectious diseases, such as parasitic diseases in which the parasite's life cycle does not include direct host-to-host transmission.

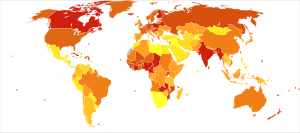
Disease burden is the impact of a health problem as measured by financial cost, mortality, morbidity, or other indicators. It is often quantified in terms of quality-adjusted life years (QALYs) or disability-adjusted life years (DALYs). Both of these metrics quantify the number of years lost due to disability (YLDs), sometimes also known as years lost due to disease or years lived with disability/disease. One DALY can be thought of as one year of healthy life lost, and the overall disease burden can be thought of as a measure of the gap between current health status and the ideal health status. According to an article published in The Lancet in June 2015, low back pain and major depressive disorder were among the top ten causes of YLDs and were the cause of more health loss than diabetes, chronic obstructive pulmonary disease, and asthma combined. The study based on data from 188 countries, considered to be the largest and most detailed analysis to quantify levels, patterns, and trends in ill health and disability, concluded that "the proportion of disability-adjusted life years due to YLDs increased globally from 21.1% in 1990 to 31.2% in 2013." The environmental burden of disease is defined as the number of DALYs that can be attributed to environmental factors. Similarly, the work-related burden of disease is defined as the number of deaths and DALYs that can be attributed to occupational risk factors to human health. These measures allow for comparison of disease burdens, and have also been used to forecast the possible impacts of health interventions. By 2014, DALYs per head were "40% higher in low-income and middle-income regions."

Balance in biomechanics, is an ability to maintain the line of gravity of a body within the base of support with minimal postural sway. Sway is the horizontal movement of the centre of gravity even when a person is standing still. A certain amount of sway is essential and inevitable due to small perturbations within the body or from external triggers. An increase in sway is not necessarily an indicator of dysfunctional balance so much as it is an indicator of decreased sensorimotor control.

Health in Ethiopia has improved markedly since the early 2000s, with government leadership playing a key role in mobilizing resources and ensuring that they are used effectively. A central feature of the sector is the priority given to the Health Extension Programme, which delivers cost-effective basic services that enhance equity and provide care to millions of women, men and children. The development and delivery of the Health Extension Program, and its lasting success, is an example of how a low-income country can still improve access to health services with creativity and dedication.

Falls in older adults are a significant cause of morbidity and mortality and are a major class of preventable injuries. Falling is one of the most common accidents that cause a loss in the quality of life for older adults, and is usually precipitated by a loss of balance and weakness in the legs. The cause of falling in old age is often multifactorial and may require a multidisciplinary approach both to treat any injuries sustained and to prevent future falls. Falls include dropping from a standing position or from exposed positions such as those on ladders or stepladders. The severity of injury is generally related to the height of the fall. The state of the ground surface onto which the victim falls is also important, harder surfaces causing more severe injury. Falls can be prevented by ensuring that carpets are tacked down, that objects like electric cords are not in one's path, that hearing and vision are optimized, dizziness is minimized, alcohol intake is moderated and that shoes have low heels or rubber soles.

Preventable causes of death are causes of death related to risk factors which could have been avoided. The World Health Organization has traditionally classified death according to the primary type of disease or injury. However, causes of death may also be classified in terms of preventable risk factors—such as smoking, unhealthy diet, sexual behavior, and reckless driving—which contribute to a number of different diseases. Such risk factors are usually not recorded directly on death certificates, although they are acknowledged in medical reports.

The Institute for Health Metrics and Evaluation (IHME) is a national and international public health agency and research institute working in the area of global health statistics and impact evaluation, located at the University of Washington in Seattle. IHME is headed by Christopher J.L. Murray, a physician, health economist, and global health researcher, and professor at the University of Washington Department of Global Health, which is part of the School of Medicine. IHME conducts research and trains scientists, policymakers, and the public in health metrics concepts, methods, and tools. Its mission includes judging the effectiveness and efficacy of health initiatives and national health systems. IHME also trains students at the post-baccalaureate and post-graduate levels.

Geriatric trauma refers to a traumatic injury that occurs to an elderly person. People around the world are living longer than ever. In developed and underdeveloped countries, the pace of population aging is increasing. By 2050, the world's population aged 60 years and older is expected to total 2 billion, up from 900 million in 2015. While this trend presents opportunities for productivity and additional experiences, it also comes with its own set of challenges for health systems. More so than ever, elderly populations are presenting to the Emergency Department following traumatic injury. In addition, given advances in the management of chronic illnesses, more elderly adults are living active lifestyles and are at risk of traumatic injury. In the United States, this population accounts for 14% of all traumatic injuries, of which a majority are just mainly from falls.
Occupational cardiovascular diseases (CVD) are diseases of the heart or blood vessels caused by working conditions, making them a form of occupational illness. These diseases include coronary heart disease, stroke, cardiomyopathy, arrythmia, and heart valve or heart chamber problems. Cardiovascular disease is the leading cause of death in the United States and worldwide. In the United States, cardiovascular diseases account for one out of four deaths. The 6th International Conference on Work Environment and Cardiovascular Diseases found that within the working age population about 10-20% of cardiovascular disease deaths can be attributed to work. Ten workplace stressors and risk factors were estimated to be associated with 120,000 U.S. deaths each year and account for 5-8% of health care costs.

Thurmon E. Lockhart is an American biomedical engineer, researcher and educator. He is the Inaugural MORE Foundation Professor of Life in Motion at Arizona State University, a guest professor at Ghent University in Belgium and, serves as a research affiliate faculty at Mayo Clinic College of Medicine and Science. He is an associate editor of Annals of Biomedical Engineering and academic and guest editor of the Sensors journal He has worked significantly to bring research to practice with various businesses to reduce falls.