Related Research Articles

The thalamus is a large mass of gray matter located in the dorsal part of the diencephalon. Nerve fibers project out of the thalamus to the cerebral cortex in all directions, known as the thalamocortical radiations, allowing hub-like exchanges of information. It has several functions, such as the relaying of sensory signals, including motor signals to the cerebral cortex and the regulation of consciousness, sleep, and alertness.
Blindsight is the ability of people who are cortically blind to respond to visual stimuli that they do not consciously see due to lesions in the primary visual cortex, also known as the striate cortex or Brodmann Area 17. The term was coined by Lawrence Weiskrantz and his colleagues in a paper published in a 1974 issue of Brain. A previous paper studying the discriminatory capacity of a cortically blind patient was published in Nature in 1973. The assumed existence of blindsight is controversial, with some arguing that it is merely degraded conscious vision.

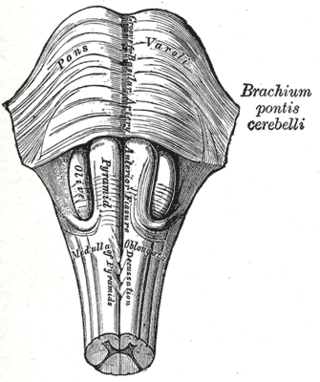
The brainstem is the stalk-like part of the brain that interconnects the cerebrum and diencephalon with the spinal cord. In the human brain, the brainstem is composed of the midbrain, the pons, and the medulla oblongata. The midbrain is continuous with the thalamus of the diencephalon through the tentorial notch.
The trochlear nerve, also known as the fourth cranial nerve, cranial nerve IV, or CN IV, is a cranial nerve that innervates a single muscle - the superior oblique muscle of the eye. Unlike most other cranial nerves, the trochlear nerve is exclusively a motor nerve.

In neuroanatomy, the lateral geniculate nucleus is a structure in the thalamus and a key component of the mammalian visual pathway. It is a small, ovoid, ventral projection of the thalamus where the thalamus connects with the optic nerve. There are two LGNs, one on the left and another on the right side of the thalamus. In humans, both LGNs have six layers of neurons alternating with optic fibers.
Visual release hallucinations, also known as Charles Bonnet syndrome or CBS, are a type of psychophysical visual disturbance in which a person with partial or severe blindness experiences visual hallucinations.
The pulvinar nuclei or nuclei of the pulvinar are the nuclei located in the thalamus. As a group they make up the collection called the pulvinar of the thalamus, usually just called the pulvinar.
In the anatomy of the brain, the centromedian nucleus, also known as the centrum medianum, is a part of the intralaminar thalamic nuclei (ITN) in the thalamus. There are two centromedian nuclei arranged bilaterally.

In neuroanatomy, the pretectal area, or pretectum, is a midbrain structure composed of seven nuclei and comprises part of the subcortical visual system. Through reciprocal bilateral projections from the retina, it is involved primarily in mediating behavioral responses to acute changes in ambient light such as the pupillary light reflex, the optokinetic reflex, and temporary changes to the circadian rhythm. In addition to the pretectum's role in the visual system, the anterior pretectal nucleus has been found to mediate somatosensory and nociceptive information.

The reticular formation is a set of interconnected nuclei that are located throughout the brainstem. It is not anatomically well defined, because it includes neurons located in different parts of the brain. The neurons of the reticular formation make up a complex set of networks in the core of the brainstem that extend from the upper part of the midbrain to the lower part of the medulla oblongata. The reticular formation includes ascending pathways to the cortex in the ascending reticular activating system (ARAS) and descending pathways to the spinal cord via the reticulospinal tracts.
Central neurogenic hyperventilation (CNH) is an abnormal pattern of breathing characterized by deep and rapid breaths at a rate of at least 25 breaths per minute. Increasing irregularity of this respiratory rate generally is a sign that the patient will enter into coma. CNH is unrelated to other forms of hyperventilation, like Kussmaul's respirations. CNH is the human body's response to reduced carbon dioxide levels in the blood. This reduction in carbon dioxide is caused by contraction of cranial arteries from damage caused by lesions in the brain stem. However, the mechanism by which CNH arises as a result from these lesions is still very poorly understood. Current research has yet to provide an effective means of treatment for the rare number of patients who are diagnosed with this condition.

In neuroanatomy, thalamocortical radiations also known as thalamocortical fibres, are the efferent fibres that project from the thalamus to distinct areas of the cerebral cortex. They form fibre bundles that emerge from the lateral surface of the thalamus.
The posterior cerebral artery (PCA) is one of a pair of cerebral arteries that supply oxygenated blood to the occipital lobe, part of the back of the human brain. The two arteries originate from the distal end of the basilar artery, where it bifurcates into the left and right posterior cerebral arteries. These anastomose with the middle cerebral arteries and internal carotid arteries via the posterior communicating arteries.

Parinaud's syndrome is a constellation of neurological signs indicating injury to the dorsal midbrain. More specifically, compression of the vertical gaze center at the rostral interstitial nucleus of medial longitudinal fasciculus (riMLF).
The zona incerta (ZI) is a horizontally elongated region of gray matter in the subthalamus below the thalamus. Its connections project extensively over the brain from the cerebral cortex down into the spinal cord.
Intention tremor is a dyskinetic disorder characterized by a broad, coarse, and low-frequency tremor evident during deliberate and visually-guided movement. An intention tremor is usually perpendicular to the direction of movement. When experiencing an intention tremor, one often overshoots or undershoots one's target, a condition known as dysmetria. Intention tremor is the result of dysfunction of the cerebellum, particularly on the same side as the tremor in the lateral zone, which controls visually guided movements. Depending on the location of cerebellar damage, these tremors can be either unilateral or bilateral.
Utilization behavior (UB) is a type of neurobehavioral phenomena that involves someone grabbing objects in view and starting the 'appropriate' behavior associated with it at an 'inappropriate' time. Patients exhibiting utilization behavior have difficulty resisting the impulse to operate or manipulate objects which are in their visual field and within reach. Characteristics of UB include unintentional, unconscious actions triggered by the immediate environment. The unpreventable excessive behavior has been linked to lesions in the frontal lobe. UB has also been referred to as "bilateral magnetic apraxia" and "hypermetamorphosis".
Conjugate gaze palsies are neurological disorders affecting the ability to move both eyes in the same direction. These palsies can affect gaze in a horizontal, upward, or downward direction. These entities overlap with ophthalmoparesis and ophthalmoplegia.
Prosopometamorphopsia is a visual disorder characterized by altered perceptions of faces. Facial features are distorted in a variety of ways including drooping, swelling, discoloration, and shifts of position. Prosopometamorphopsia is distinct from prosopagnosia which is characterised by the inability to recognise faces. About 75 cases of prosopometamorphopsia have been reported in the scientific literature. In about half of the reported cases, features on both sides of the face appear distorted. In the other half of cases, distortions are restricted to one side of the face and this condition is called hemi-prosopometamorphopsia.

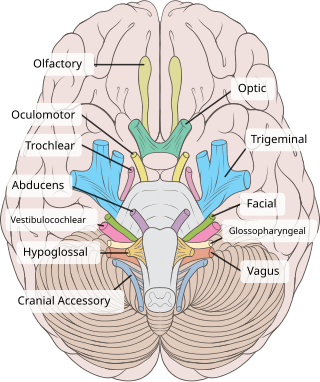
The visual pathway consists of structures that carry visual information from the retina to the brain. Lesions in that pathway cause a variety of visual field defects. In the visual system of human eye, the visual information processed by retinal photoreceptor cells travel in the following way:
Retina→Optic nerve→Optic chiasma →Optic tract→Lateral geniculate body→Optic radiation→Primary visual cortex
References
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 Mocellin, Ramon; Walterfang, Mark; Velakoulis, Dennis (September 2006). "Neuropsychiatry of complex visual hallucinations". The Australian and New Zealand Journal of Psychiatry. 40 (9): 742–751. doi:10.1080/j.1440-1614.2006.01878.x. ISSN 0004-8674. PMID 16911748. S2CID 12151224.
- ↑ Benke, Thomas (2006). "Peduncular hallucinosis". Journal of Neurology. 253 (12): 1561–1571. doi:10.1007/s00415-0060-0254-4. PMID 17006630. S2CID 25990312.
- 1 2 3 4 Kumar, R., Wahi, J., Banerji, D., & Sharma, K. (1999). Peduncular Hallucinosis: An Unusual Sequel to Surgical Intervention in the Suprasellar Region. British Journal of Neurosurgery, 13(5), 500-503.
- 1 2 3 Benke, T. (2006). Peduncular Hallucinosis - a Syndrome of Impaired Reality Monitoring. Journal of Neurology, 253(12), 1561-1571.
- 1 2 3 FEINBERG W, M., & RAPCSAK S, Z. (1989). Peduncular Hallucinosis Following Paramedian Thalamic Infarction. Neurology, 39(11), 1535-1536.
- 1 2 3 4 Spiegel, D., Eastern Virginia Medical School Dept. of Psychiatry, interviewed by C. Byars, Oct. 12, 2009.
- ↑ Howlett, D., Downie, A., Banerjee, A., Tonge, K., & Oakeley, H. (1994). MRI of an Unusual Case of Peduncular Hallucinosis (Lhermitte's Syndrome). Neuroradiology, 36(2), 121-122.