Related Research Articles
Immunotherapy or biological therapy is the treatment of disease by activating or suppressing the immune system. Immunotherapies designed to elicit or amplify an immune response are classified as activation immunotherapies, while immunotherapies that reduce or suppress are classified as suppression immunotherapies. Immunotherapy is under preliminary research for its potential to treat various forms of cancer.
A cancer vaccine, or oncovaccine, is a vaccine that either treats existing cancer or prevents development of cancer. Vaccines that treat existing cancer are known as therapeutic cancer vaccines or tumor antigen vaccines. Some of the vaccines are "autologous", being prepared from samples taken from the patient, and are specific to that patient.
Cancer immunotherapy (immuno-oncotherapy) is the stimulation of the immune system to treat cancer, improving the immune system's natural ability to fight the disease. It is an application of the fundamental research of cancer immunology and a growing subspecialty of oncology.
An oncolytic virus is a virus that preferentially infects and kills cancer cells. As the infected cancer cells are destroyed by oncolysis, they release new infectious virus particles or virions to help destroy the remaining tumour. Oncolytic viruses are thought not only to cause direct destruction of the tumour cells, but also to stimulate host anti-tumour immune system responses. Oncolytic viruses also have the ability to affect the tumor micro-environment in multiple ways.
An angiogenesis inhibitor is a substance that inhibits the growth of new blood vessels (angiogenesis). Some angiogenesis inhibitors are endogenous and a normal part of the body's control and others are obtained exogenously through pharmaceutical drugs or diet.
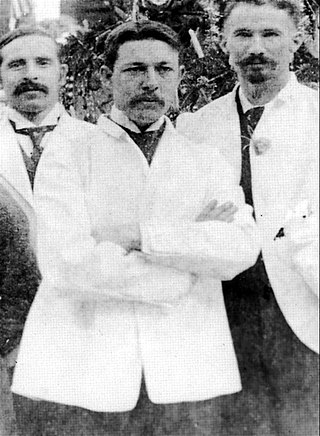
William Bradley Coley was an American bone surgeon and cancer researcher best known for his early contributions to the study of cancer immunotherapy, specifically causing infection as a way to fight cancer, a practice used as far back as 1550 BC. His work was not proven effective in his lifetime, and today Coley's toxins are known to be both ineffective and potentially harmful. Coley is nevertheless recognized as the Father of Cancer Immunotherapy for his contributions to the science.
Coley's toxins is a mixture containing toxins filtered from killed bacteria of species Streptococcus pyogenes and Serratia marcescens, named after William Coley, a surgical oncologist at the Hospital for Special Surgery who developed the mixture in the late 19th century as a treatment for cancer.
The following are notable events in the Timeline of immunology:

Steven A. Rosenberg is an American cancer researcher and surgeon, chief of Surgery at the National Cancer Institute in Bethesda, Maryland and a Professor of Surgery at the Uniformed Services University of Health Sciences and the George Washington University School of Medicine and Health Sciences. He pioneered the development of immunotherapy that has resulted in the first effective immunotherapies and the development of gene therapy. He is the first researcher to successfully insert foreign genes into humans.
Cancer immunology (immuno-oncology) is an interdisciplinary branch of biology and a sub-discipline of immunology that is concerned with understanding the role of the immune system in the progression and development of cancer; the most well known application is cancer immunotherapy, which utilises the immune system as a treatment for cancer. Cancer immunosurveillance and immunoediting are based on protection against development of tumors in animal systems and (ii) identification of targets for immune recognition of human cancer.

Programmed death-ligand 1 (PD-L1) also known as cluster of differentiation 274 (CD274) or B7 homolog 1 (B7-H1) is a protein that in humans is encoded by the CD274 gene.
Gamma delta T cells are T cells that have a γδ T-cell receptor (TCR) on their surface. Most T cells are αβ T cells with TCR composed of two glycoprotein chains called α (alpha) and β (beta) TCR chains. In contrast, γδ T cells have a TCR that is made up of one γ (gamma) chain and one δ (delta) chain. This group of T cells is usually less common than αβ T cells. Their highest abundance is in the gut mucosa, within a population of lymphocytes known as intraepithelial lymphocytes (IELs).
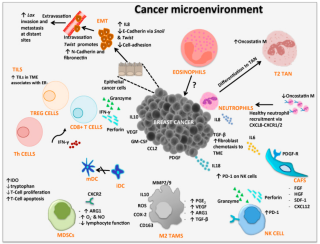
Tumor-associated macrophages (TAMs) are a class of immune cells present in high numbers in the microenvironment of solid tumors. They are heavily involved in cancer-related inflammation. Macrophages are known to originate from bone marrow-derived blood monocytes or yolk sac progenitors, but the exact origin of TAMs in human tumors remains to be elucidated. The composition of monocyte-derived macrophages and tissue-resident macrophages in the tumor microenvironment depends on the tumor type, stage, size, and location, thus it has been proposed that TAM identity and heterogeneity is the outcome of interactions between tumor-derived, tissue-specific, and developmental signals.
Cytokine-induced killer cells (CIK) cells are a group of immune effector cells featuring a mixed T- and natural killer (NK) cell-like phenotype. They are generated by ex vivo incubation of human peripheral blood mononuclear cells (PBMC) or cord blood mononuclear cells with interferon-gamma (IFN-γ), anti-CD3 antibody, recombinant human interleukin (IL)-1 and recombinant human interleukin (IL)-2.
Hua Eleanor Yu is the inaugural Billy and Audrey L. Wilder Professor in tumor immunotherapy at the Beckman Research Institute of the City of Hope National Medical Center in Duarte, California. In addition, she co-leads the Cancer Immunotherapeutics Program at the City of Hope cancer center, with Peter P. Lee. Yu's laboratory was the first to identify STAT3, a protein that helps to protect tumor cells from the immune system. Her group is developing possible drug treatments using CpG-Stat3 siRNA to attack tumor cells in mice and humans.
Cryoimmunotherapy, also referred to as cryoimmunology, is an oncological treatment for various cancers that combines cryoablation of tumor with immunotherapy treatment. In-vivo cryoablation of a tumor, alone, can induce an immunostimulatory, systemic anti-tumor response, resulting in a cancer vaccine—the abscopal effect. Thus, cryoablation of tumors is a way of achieving autologous, in-vivo tumor lysate vaccine and treat metastatic disease. However, cryoablation alone may produce an insufficient immune response, depending on various factors, such as high freeze rate. Combining cryotherapy with immunotherapy enhances the immunostimulating response and has synergistic effects for cancer treatment.
Gabriel A. Rabinovich is an Argentine biochemist who is currently a professor at the School of Exact and Natural Sciences at the University of Buenos Aires. He is also the deputy director of Immunopathology Laboratories, and the head of Structural and Functional Glycomic Laboratories.

Michele 'Miki' De Palma is an Italian biologist and a professor at EPFL. He is known for his work on the role of macrophages in cancer progression and the discovery of Tie2-expressing angiogenic monocytes.

George Coukos is a physician-scientist in tumor immunology, professor and director of the Ludwig Cancer Research Lausanne Branch and director of the Department of oncology UNIL-CHUV of the University of Lausanne and the Lausanne University Hospital in Lausanne, Switzerland. He is known for his work on the mechanisms by which tumors suppress anti-cancer immune responses, and the role of the tumor vasculature in that suppression. In addition to his work in ovarian cancer, the combinatorial immune therapies proposed by Professor Coukos have been successfully tested and approved for lung, liver and kidney cancers.

Endothelial cell anergy is a condition during the process of angiogenesis, where endothelial cells, the cells that line the inside of blood vessels, can no longer respond to inflammatory cytokines. These cytokines are necessary to induce the expression of cell adhesion molecules to allow leukocyte infiltration from the blood into the tissue at places of inflammation, such as a tumor. This condition, which protects the tumor from the immune system, is the result of exposure to angiogenic growth factors.
References
- ↑ Radha G., Lopus M. (2021) The spontaneous remission of cancer: Current insights and therapeutic significance. Translational Oncology. 14 (9):101166, doi:10.1016/j.tranon.2021.101166
- 1 2 3 Everson T., Cole W. (1968) Spontaneous Regression of Cancer Philadelphia, JB Saunder & Co (Book)
- 1 2 3 Hobohm, U. (2001). "Fever and cancer in perspective". Cancer Immunology, Immunotherapy. 50 (8): 391–6. doi:10.1007/s002620100216. PMID 11726133. S2CID 109998.
- ↑ Zahl, P. H.; Maehlen, J.; Welch, H. G. (2008). "The natural history of invasive breast cancers detected by screening mammography". Archives of Internal Medicine. 168 (21): 2311–6. doi:10.1001/archinte.168.21.2311. PMID 19029493.
- 1 2 Challis, G. B.; Stam, H. J. (1990). "The spontaneous regression of cancer. A review of cases from 1900 to 1987". Acta Oncologica. 29 (5): 545–50. doi: 10.3109/02841869009090048 . PMID 2206563.
- ↑ Robert A. Weinberg (2007) The Biology of Cancer, Garland Science
- ↑ Hobohm, U. (2005). "Fever therapy revisited". British Journal of Cancer. 92 (3): 421–5. doi:10.1038/sj.bjc.6602386. PMC 2362074 . PMID 15700041.
- ↑ Hobohm, U.; Stanford, J. L.; Grange, J. M. (2008). "Pathogen-associated molecular pattern in cancer immunotherapy". Critical Reviews in Immunology. 28 (2): 95–107. doi:10.1615/critrevimmunol.v28.i2.10. PMID 18540826.
- ↑ Maletzki, C.; Linnebacher, M.; Savai, R.; Hobohm, U. (2013). "Mistletoe lectin has a shiga toxin-like structure and should be combined with other Toll-like receptor ligands in cancer therapy" (PDF). Cancer Immunology, Immunotherapy. 62 (8): 1283–92. doi:10.1007/s00262-013-1455-1. PMID 23832140. S2CID 26031460.
- ↑ Rohdenburg, G. L. (1 April 1918). "Fluctuations in the Growth Energy of Malignant Tumors in Man, with Especial Reference to Spontaneous Recession". The Journal of Cancer Research. 3 (2): 193–225. doi:10.1158/jcr.1918.193 (inactive 31 January 2024).
{{cite journal}}: CS1 maint: DOI inactive as of January 2024 (link) - ↑ Fauvet, J.; Roujeau, J.; Piet, R. (1964). "Spontaneous Cancer Cures and Regressions". La Revue du Praticien. 14: 2177–80. PMID 14157391.
- ↑ Boyd W: The spontaneous regression of cancer. Charles Thomas, Publ., Springfield Ill. 1966 (Book)
- ↑ Cole, W. H. (1976). "Spontaneous regression of cancer and the importance of finding its cause". National Cancer Institute Monograph. 44: 5–9. PMID 799760.
- ↑ O'Regan, Brendan; Hirschberg, Carlyle (1993). Spontaneous Remission. An Annotated Bibliography. Sausalito, California: Institute of Noetic Sciences. ISBN 978-0-943951-17-1.
- ↑ Turner, Kelly Ann (2010). Spontaneous Remission of Cancer: Theories from Healers, Physicians, and Cancer Survivors (Thesis). Berkeley: UC Berkeley Electronic Theses and Dissertations.
- ↑ Geoggrey Cowley (March 13, 1995). "Surviving Against All Odds". Newsweek . p. 63.
- ↑ Caryle Hirshberg; Marc Ian Barasch (1996). Remarkable Recovery. Riverhead Books. ISBN 9781573225304.