
The T sets, also referred to as the Tangara trains, are a class of electric multiple units that currently operate on the Sydney Trains network. Built by A Goninan & Co, the sets entered service between 1988 and 1995, initially under the State Rail Authority and later on CityRail. The T sets were built as "third-generation" trains for Sydney's rail fleet, coinciding with the final withdrawals of the "Red Rattler" sets from service in the late 1980s and early 1990s. The Tangaras were initially built as two classes; the long-distance G sets and the suburban T sets, before being merged after successive refurbishments.

A dead man's switch is a switch that is designed to be activated or deactivated if the human operator becomes incapacitated, such as through death, loss of consciousness, or being bodily removed from control. Originally applied to switches on a vehicle or machine, it has since come to be used to describe other intangible uses, as in computer software.

On trains, the expression emergency brake has several meanings:
The Train Protection & Warning System (TPWS) is a train protection system used throughout the British passenger main-line railway network, and in Victoria, Australia.
The town of Morpeth in Northumberland, England, has what is reputed to be the tightest curve of any main railway line in Britain. The track turns approximately 98° from a northwesterly to an easterly direction immediately west of Morpeth Station on an otherwise fast section of the East Coast Main Line railway. This was a major factor in three serious derailments between 1969 and 1994. The curve has a permanent speed restriction of 50 miles per hour (80 km/h).

The Southall rail crash occurred on 19 September 1997, on the Great Western Main Line at Southall, West London. An InterCity 125 high speed passenger train (HST) failed to slow down in response to warning signals and collided with a freight train crossing its path, causing seven deaths and 139 injuries.

The Nuneaton rail crash occurred on 6 June 1975, on the West Coast Main Line just south of Nuneaton railway station in Warwickshire, England, United Kingdom.
On 8 February 1986, twenty-three people were killed in a collision between a Canadian National Railway freight train and a Via Rail passenger train called the Super Continental, including the engine crews of both trains. It was the deadliest rail disaster in Canada since the Dugald accident of 1947, which had thirty-one fatalities, and was not surpassed until the Lac-Mégantic rail disaster in 2013, which resulted in 47 deaths.

The Amagasaki derailment occurred in Amagasaki, Hyōgo Prefecture, Japan, on 25 April 2005 at 09:19 local time, just after the local rush hour. It occurred when a seven-car commuter train came off the tracks on West Japan Railway Company's Fukuchiyama Line in just before Amagasaki on its way for Dōshisha-mae via the JR Tōzai Line and the Gakkentoshi Line, and the front two cars rammed into an apartment building. The first car slid into the first-floor parking garage and as a result took days to remove, while the second slammed into the corner of the building, being crushed into an L-shaped against it by the weight of the remaining cars. Of the roughly 700 passengers on board at the time of the crash, 106 passengers, in addition to the driver, were killed and 562 others injured. Most survivors and witnesses claimed that the train appeared to have been travelling too fast. The incident was Japan's most serious since the 1963 Tsurumi rail accident.

The South Coast Line (SCO) is an intercity rail service operated by NSW TrainLink that services the Illawarra region of New South Wales, Australia. The service runs from Central, and runs the entire length of the eponymous South Coast railway line to Bomaderry. The service also runs along the Eastern Suburbs railway line at peak hours and the Port Kembla railway line to Port Kembla. It is operated with NSW TrainLink H sets and Sydney Trains T sets, with Endeavour railcars operating the service on the non-electrified line between Kiama and Bomaderry.

Mendip Rail Ltd is an independent freight operating railway company in Great Britain. It is a joint venture composed of the rail-operation divisions of Aggregate Industries and Hanson Aggregates.
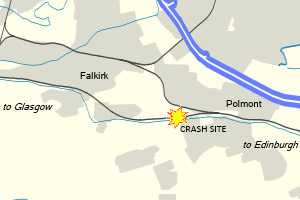
The Polmont rail accident, also known as the Polmont rail disaster, occurred on 30 July 1984 to the west of Polmont, near Falkirk, in Scotland. A westbound push-pull express train travelling from Edinburgh to Glasgow struck a cow which had gained access to the track through a damaged fence from a field near Polmont railway station, causing all six carriages and the locomotive of the train to derail. 13 people were killed and 61 others were injured, 17 of them seriously. The accident led to a debate about the safety of push-pull trains on British Rail.
The railways of New South Wales, Australia have had many incidents and accidents since their formation in 1831. There are close to 1000 names associated with rail-related deaths in NSW on the walls of the Australian Railway Monument in Werris Creek. Those killed were all employees of various NSW railways. The details below include deaths of employees and the general public.

The Cairns Tilt Train derailment occurred at 11:55 pm on 15 November 2004 when the City of Townsville diesel tilt train derailed north of Berajondo, approximately 342 km (213 mi) northwest of Brisbane, the state capital of Queensland, Australia.

Sifa is a type of deadman's control system used on German-influenced European railways. Although deadman's pedals are commonly used on railways worldwide, Sifa systems are specifically those codified by German Industrial Norms VDE 0119-207-5.
The Halle train collision was a collision between two NMBS/SNCB passenger trains carrying a combined 250 to 300 people in Buizingen, in the municipality of Halle, Flemish Brabant, Belgium, on 15 February 2010. The accident occurred in snowy conditions at 08:28 CET (07:28 UTC), during rush hour, on railway line 96 (Brussels–Quévy) about 12 kilometres (7.5 mi) from Brussels between P-train E3678 from Leuven to Braine-le-Comte and IC-train E1707 from Quiévrain to Liège. A third train was able to come to a stop just in time. The collision killed 19 people and injured 171, making it the deadliest rail accident in Belgium in over fifty years.

On 9 November 2016, a tram operated by Tramlink derailed and overturned on a sharp bend approaching a junction. Of 69 passengers, there were seven fatalities and 62 injured, 19 of whom sustained serious injuries. This was the first tram incident in the United Kingdom in which passengers died since 1959.
On 3 February 2003, a Comeng electric multiple unit train rolled away from Broadmeadows station in Melbourne, Australia, before it ran for nearly 17 kilometres (11 mi) out of control without a driver and eventually crashed into another train about to depart Spencer Street station. Train controllers attempted several times to stop or redirect the train, but were limited in their ability to intervene, instead being forced to alter the route of other trains to avert a more serious collision. Eleven people on board the stationary train were injured; authorities did not know until after the crash if any passengers were on board the runaway. An investigation identified driver error as the cause of the accident, but the runaway event prompted significant debate about the role of government authorities and private operators in ensuring safety and reliability on the Melbourne rail network.

On 20 February 2020, a NSW TrainLink XPT passenger train derailed while passing through a turnout at Wallan, Victoria, Australia. Of the 162 total on board, there were two fatalities and 61 passengers were injured, eight of whom sustained serious injuries.

The Salisbury Rail Crash was a railway accident on 31 October 2021, at Salisbury, Wiltshire, United Kingdom. Two trains, travelling on converging lines, collided at Salisbury Tunnel Junction, approximately one mile northeast of Salisbury railway station. Fourteen people, including one of the train drivers, were taken to hospital.
