Veins are blood vessels in the circulatory system of humans and most other animals that carry blood towards the heart. Most veins carry deoxygenated blood from the tissues back to the heart; exceptions are those of the pulmonary and fetal circulations which carry oxygenated blood to the heart. In the systemic circulation, arteries carry oxygenated blood away from the heart, and veins return deoxygenated blood to the heart, in the deep veins.
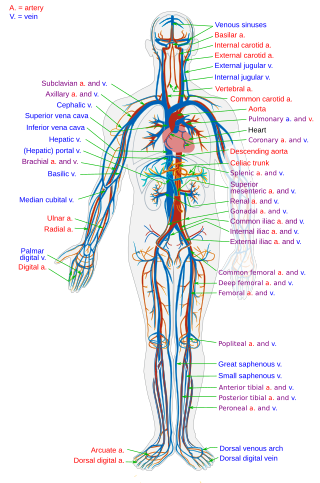
The circulatory system is a system of organs that includes the heart, blood vessels, and blood which is circulated throughout the entire body of a human or other vertebrate. It includes the cardiovascular system, or vascular system, that consists of the heart and blood vessels. The circulatory system has two divisions, a systemic circulation or circuit, and a pulmonary circulation or circuit. Some sources use the terms cardiovascular system and vascular system interchangeably with circulatory system.

Coronary artery bypass surgery, also known as coronary artery bypass graft, is a surgical procedure to treat coronary artery disease (CAD), the buildup of plaques in the arteries of the heart. It can relieve chest pain caused by CAD, slow the progression of CAD, and increase life expectancy. It aims to bypass narrowings in heart arteries by using arteries or veins harvested from other parts of the body, thus restoring adequate blood supply to the previously ischemic heart.

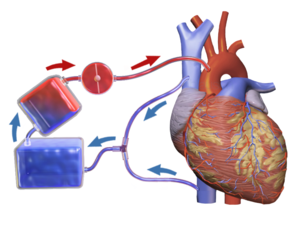
Extracorporeal membrane oxygenation (ECMO), is a form of extracorporeal life support, providing prolonged cardiac and respiratory support to persons whose heart and lungs are unable to provide an adequate amount of oxygen, gas exchange or blood supply (perfusion) to sustain life. The technology for ECMO is largely derived from cardiopulmonary bypass, which provides shorter-term support with arrested native circulation. The device used is a membrane oxygenator, also known as an artificial lung.

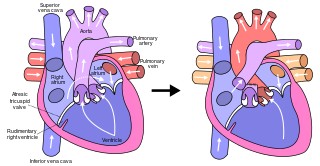
dextro-Transposition of the great arteries is a potentially life-threatening birth defect in the large arteries of the heart. The primary arteries are transposed.
A cyanotic heart defect is any congenital heart defect (CHD) that occurs due to deoxygenated blood bypassing the lungs and entering the systemic circulation, or a mixture of oxygenated and unoxygenated blood entering the systemic circulation. It is caused by structural defects of the heart such as right-to-left or bidirectional shunting, malposition of the great arteries, or any condition which increases pulmonary vascular resistance. The result may be the development of collateral circulation.
The Fontan procedure or Fontan–Kreutzer procedure is a palliative surgical procedure used in children with univentricular hearts. It involves diverting the venous blood from the inferior vena cava (IVC) and superior vena cava (SVC) to the pulmonary arteries. The procedure varies for differing congenital heart pathologies. For example in tricuspid atresia, the procedure can be done where the blood does not pass through the morphologic right ventricle; i.e., the systemic and pulmonary circulations are placed in series with the functional single ventricle. Whereas in hypoplastic left heart syndrome, the heart is more reliant on the more functional right ventricle to provide blood flow to the systemic circulation. The procedure was initially performed in 1968 by Francis Fontan and Eugene Baudet from Bordeaux, France, published in 1971, simultaneously described in July 1971 by Guillermo Kreutzer from Buenos Aires, Argentina, presented at the Argentinean National Cardilogy meeting of that year and finally published in 1973.
A cardiovascular perfusionist, clinical perfusionist or perfusiologist, and occasionally a cardiopulmonary bypass doctor or clinical perfusion scientist, is a healthcare professional who operates the cardiopulmonary bypass machine during cardiac surgery and other surgeries that require cardiopulmonary bypass to manage the patient's physiological status. As a member of the cardiovascular surgical team, the perfusionist also known as the clinical perfusionist helps maintain blood flow to the body's tissues as well as regulate levels of oxygen and carbon dioxide in the blood, using a heart–lung machine.

The atrium is one of the two upper chambers in the heart that receives blood from the circulatory system. The blood in the atria is pumped into the heart ventricles through the atrioventricular mitral and tricuspid heart valves.

Arterial switch operation (ASO) or arterial switch, is an open heart surgical procedure used to correct dextro-transposition of the great arteries (d-TGA).

In thoracic surgery, a pulmonary thromboendarterectomy (PTE), also referred to as pulmonary endarterectomy (PEA), is an operation that removes organized clotted blood (thrombus) from the pulmonary arteries, which supply blood to the lungs.
Cardioplegia is a solution given to the heart during cardiac surgery, to minimize the damage caused by myocardial ischemia while the heart is paused.
A cardiac shunt is a pattern of blood flow in the heart that deviates from the normal circuit of the circulatory system. It may be described as right-left, left-right or bidirectional, or as systemic-to-pulmonary or pulmonary-to-systemic. The direction may be controlled by left and/or right heart pressure, a biological or artificial heart valve or both. The presence of a shunt may also affect left and/or right heart pressure either beneficially or detrimentally.

An oxygenator is a medical device that is capable of exchanging oxygen and carbon dioxide in the blood of human patients during surgical procedures that may necessitate the interruption or cessation of blood flow in the body, a critical organ or great blood vessel. These organs can be the heart, lungs or liver, while the great vessels can be the aorta, pulmonary artery, pulmonary veins or vena cava.

The bidirectional Glenn (BDG) shunt, or bidirectional cavopulmonary anastomosis, is a surgical technique used in pediatric cardiac surgery procedure used to temporarily improve blood oxygenation for patients with a congenital cardiac defect resulting in a single functional ventricle. Creation of a bidirectional shunt reduces the amount of blood volume that the heart needs to pump at the time of surgical repair with the Fontan procedure.
Cardiothoracic anesthesiology is a subspeciality of the medical practice of anesthesiology, devoted to the preoperative, intraoperative, and postoperative care of adult and pediatric patients undergoing cardiothoracic surgery and related invasive procedures.
The Senning procedure is an atrial switch heart operation performed to treat transposition of the great arteries. It is named after its inventor, the Swedish cardiac surgeon Åke Senning (1915–2000), also known for implanting the first permanent cardiac pacemaker in 1958.
Extracorporeal cardiopulmonary resuscitation is a method of cardiopulmonary resuscitation (CPR) that passes the patient's blood through a machine in a process to oxygenate the blood supply. A portable extracorporeal membrane oxygenation (ECMO) device is used as an adjunct to standard CPR. A patient who is deemed to be in cardiac arrest refractory to CPR has percutaneous catheters inserted into the femoral vein and artery. Theoretically, the application of ECPR allows for the return of cerebral perfusion in a more sustainable manner than with external compressions alone. By attaching an ECMO device to a person who has acutely undergone cardiovascular collapse, practitioners can maintain end-organ perfusion whilst assessing the potential reversal of causal pathology, with the goal of improving long-term survival and neurological outcomes.
Retrograde autologous priming (RAP) is a means to effectively and safely restrict the hemodilution caused by the direct homologous blood transfusion and reduce the blood transfusion requirements during cardiac surgery. It is also generally considered a blood conservation method used in most patients during the cardiopulmonary bypass (CPB). The processing of RAP includes three main steps, and the entire procedure of RAP could be completed within 5 to 8 minutes. This technique is proposed by Panico in 1960 for the first time and restated by Rosengart in 1998 to eliminate or reduce the risk of hemodilution during CPB. Moreover, to precisely determine the clinical efficacy of RAP, many related studies were conducted. Most results of researches indicate that RAP is available to provide some benefits to reducing the requirements for red blood cell transfusion. However, there are still some studies showing a failure of RAP to limit the hemodilution after the open heart operation.
Raghib syndrome is rare a congenital heart defect where the left superior vena cava (LSVC) is draining into the left atrium in addition to an absent coronary sinus and an atrial septal defect. This can be considered a dangerous heart condition because it puts the individual at a high risk of stroke. Other defects that are often associated with Raghib syndrome can include ventricular septal defects, enlargement of the tricuspid annulus, and pulmonary stenosis. While this is considered an extremely rare developmental complex, cases regarding a persistent left superior vena cava (PLSVC) are relatively common among congenital heart defects. It is also important to note that the PLSVC often drains into the right atrium, and only drains into the left atrium in approximately 10 to 20% of individuals with the defect.