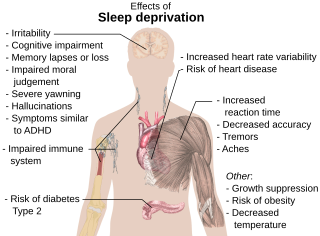
Performance errors relative to sleep loss and extended wakefulness
A meta-analysis (Category I) that was conducted by Pilcher and Huffcutt [1] examined data that were drawn from 19 research studies to characterize the effects of sleep deprivation on specific types of human performance. Motor skills, cognitive skills, and mood were assessed in terms of: partial sleep derivation (also known as sleep deprivation), which is defined as fewer than 5 hours of sleep in a 24-hour period for 1 or more days; short-term total sleep deprivation (no sleep attained for fewer than 45 hours); and long-term sleep deprivation (no sleep attained for a period in excess of 45 hours). These researchers found that sleep-deprived subjects performed considerably worse on motor tasks, cognitive tasks, and measures of mood than did non-sleep-deprived subjects. The greatest impact on cognitive performance was seen from multiple days of partial sleep deprivation, although short- and long-term sleep deprivation also showed an effect. Meta-analyses of sleep deprivation effects in medical residents found deficits in both laboratory tasks and clinical tasks. [2]
The magnitude of the chronic partial sleep loss has been experienced by astronauts in flight [3] [4] [5] [6] [7] [8] [9] has been reported to negatively impact cognitive performance in multiple Category I, Category II and Category III laboratory and field studies. [10] [11] [12] [13] [14] Performance can be affected whether sleep loss is in the form of a night of substantially reduced sleep, a night of total sleep deprivation, or a series of less drastic, but more chronic, restricted sleep hours. A 1997 study by Dinges et al. [10] revealed that when sleep is restricted to the level that is commonly experienced by astronauts, a "sleep debt" accrues and, in less than 1 week, performance deficits during waking hours reach levels of serious impairment.
Chronic reduction of sleep can impact performance in a manner that is similar to that of total sleep deprivation. A study by Van Dongen et al., [15] which used 48 subjects, evaluated the specific performance effects of chronic sleep restriction in comparison to the effects of 3 nights of total sleep deprivation. Sleep restriction conditions included 14 consecutive nights of 8, 6, or 4 hours of sleep opportunity, with actual sleep quantity validated by polysomnography recordings. Subjects who were subjected to sleep restriction conditions underwent neurobehavioral assessments every 2 hours during their scheduled wakefulness, while subjects who were subjected to the sleep deprivation condition were tested every 2 hours throughout their total 88 hours of sleep deprivation.
The neurobehavioral assessment battery that was used in the Van Dongen et al. [15] study included the psychomotor vigilance task (PVT). The PVT - which determines alertness and the effects of fatigue on cognitive performance (as determined by lapses in response time and accuracy of responses) by measuring the speed with which subjects respond to a visual or auditory stimulus (by pressing a response button) - has become a standard laboratory tool for the assessment of sustained performance in a variety of experimental conditions. [16] The PVT detects changes in basic neurobehavioral performance that involve vigilant attention, response speed, and impulsivity; and it has been extensively validated in ground-based laboratory studies to detect cognitive deficits that are caused by a variety of factors (e.g., restricted sleep, sleep/wake shifts, motion sickness, residual sedation from sleep medications). [15] [17] [18] The PVT is an optimal tool for repeated use, in contrast to some other cognitive measures, as studies have shown no minimal learning effects and aptitude differences when using the PVT. [15] [19] [20]

Results from these laboratory studies indicate that multiple consecutive sleep episodes of 4 or 6 hours significantly erode performance on the PVT and on measures of working memory, and that performance under these two conditions (i.e., 4 or 6 hours) was comparable to the performance that is found under conditions of 1 to 2 days of total sleep deprivation. Surprisingly, by the end of the 14 days of sleep restriction, subjects in the 4- and 6-hour sleep period conditions reported feeling only slightly sleepy. As these reports were taken when performance was at its lowest level, this indicates that the subjects may no longer have been aware of their performance deficits because of inadequate recovery sleep (figure 3–2). [15]
Subjects who spent 4 hours in bed reached levels of impairment at 6 days and of severe impairment at 11 days. Subjects who spent 6 hours in bed reached levels of impairment at 7 days. It appears that subjects who spent 8 hours in bed approached levels of impairment. Figure 3-3, which is from Belenky et al., [21] however, demonstrates that subjects who spent 9 hours in bed did not approach these levels of impairment, indicating that 9 hours in bed may be needed to alleviate the risk of performance errors.

Similar performance effects resulting from chronically restricted can also be seen in the Category I study by Belenky et al. [21] and in figure 3-3. This study involved 66 subjects who were observed in four conditions (i.e., 3, 5, 7 and 9 hours in bed) for 7 days. PVT testing showed severe impairments in reaction time under the 3-hour condition, with lapses in responses increasing steadily across the 7 days of sleep restriction. Subjects who spent 3 hours in bed reached levels of severe impairment at 5 days, while subjects who spent 5 hours in bed reached levels of impairment at 4 days.
These Category I laboratory studies by Van Dongen et al. [15] and Belenky et al. [21] clearly show that subjects suffered performance impairments resulting from total sleep deprivation and/or chronic sleep restriction.
Cognitive impairments are present even after an individual has been awake for approximately 17 hours; in fact, recent studies have shown that these decrements are similar to those that result from an elevated blood alcohol level. A compelling Category I laboratory study from Williamson and Feyer [22] used a cross-over randomized control design to observe cognitive and motor performance after minor sleep deprivation to performance after alcohol consumption. All subjects participated in both alcohol consumption and sleep deprivation, and the order of testing was counterbalanced so that half of the subjects participated in the alcohol consumption part first while the other half participated in the sleep deprivation part first. To avoid carry-over effects from one condition to the next, subjects were provided with a night of rest in a motel between each condition.
Results indicate that, on average, performance with a blood alcohol level of 0.05% remained equivalent to performance after being awake for 16.9 to 18.6 hours. Performance with a blood alcohol level of 0.1% was equivalent to performance after being awake for 17.7 to 19.7 hours, or to restricted sleep of 4 to 5 hours per night for 1 week. [23] Similar studies that compare performance after a time of sleep deprivation to performance with elevated blood alcohol level have confirmed these results. [24] These findings are compelling as the duration of wakefulness (17 hours), which results in decrements that are similar to those that are induced by a 0.05% blood alcohol level, is considered by many to be within the range of a "normal" waking "day"; many individuals can recall an incident in which they had to waken early in the morning and work all day into the night. Astronauts, who sleep on average of 6 hours per night, [4] [6] [7] [8] may be performing critical tasks 17 hours or more after wakening.