Related Research Articles

Cognitive behavioral therapy (CBT) is a psycho-social intervention that aims to reduce symptoms of various mental health conditions, primarily depression and anxiety disorders. CBT focuses on challenging and changing cognitive distortions and their associated behaviors to improve emotional regulation and develop personal coping strategies that target solving current problems. Though it was originally designed to treat depression, its uses have been expanded to include the treatment of many mental health conditions, including anxiety, substance use disorders, marital problems, and eating disorders. CBT includes a number of cognitive or behavioral psychotherapies that treat defined psychopathologies using evidence-based techniques and strategies.
Post-traumatic stress disorder (PTSD) is a mental and behavioral disorder that can develop because of exposure to a traumatic event, such as sexual assault, warfare, traffic collisions, child abuse, domestic violence, or other threats on a person's life. Symptoms may include disturbing thoughts, feelings, or dreams related to the events, mental or physical distress to trauma-related cues, attempts to avoid trauma-related cues, alterations in the way a person thinks and feels, and an increase in the fight-or-flight response. These symptoms last for more than a month after the event. Young children are less likely to show distress but instead may express their memories through play. A person with PTSD is at a higher risk of suicide and intentional self-harm.
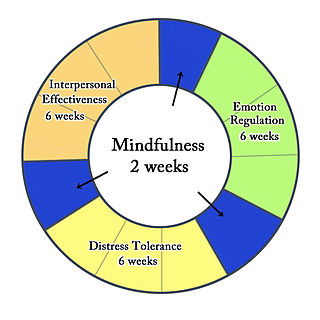
Dialectical behavior therapy (DBT) is an evidence-based psychotherapy that began with efforts to treat personality disorders and interpersonal conflicts. Evidence suggests that DBT can be useful in treating mood disorders and suicidal ideation, as well as for changing behavioral patterns such as self-harm and substance use. DBT evolved into a process in which the therapist and client work with acceptance and change-oriented strategies, and ultimately balance and synthesize them—comparable to the philosophical dialectical process of thesis and antithesis followed by synthesis.
Psychological trauma, mental trauma or psychotrauma is an emotional response to a distressing event or series of events, such as accidents, rape, or natural disasters. Reactions such as psychological shock and psychological denial are typical. Longer-term reactions include unpredictable emotions, flashbacks, difficulties with interpersonal relationships and sometimes physical symptoms including headaches or nausea.
Eye movement desensitization and reprocessing (EMDR) is a form of psychotherapy developed by Francine Shapiro in the 1980s that was originally designed to alleviate the distress associated with traumatic memories such as post-traumatic stress disorder (PTSD). In EMDR, the person being treated recalls distressing experiences whilst doing bilateral stimulation, such as side-to-side eye movement or physical stimulation, such as tapping either side of the body.
Barbara Rothbaum is a psychologist at Emory University School of Medicine in Atlanta, Georgia. She is a professor in the Psychiatry department and a pioneer in the treatment of anxiety-related disorders. Rothbaum is head of the Trauma and Anxiety Recovery Program (TARP) at Emory as well as the Emory Healthcare Veterans Program. In the mid-1990s she founded a virtual exposure therapy company called Virtually Better, Inc. This company treats patients with anxiety disorders, addictions, pain, and the like using virtual reality instead of the actual place or scenario. It also allows the therapist to control the environment. She also played a key role in the development of the treatment of posttraumatic stress disorder (PTSD).
Complex post-traumatic stress disorder is a psychological disorder that is theorized to develop in response to exposure to a series of traumatic events in a context in which the individual perceives little or no chance of escape, and particularly where the exposure is prolonged or repetitive. It is not yet recognized by the American Psychiatric Association or the DSM-5 as a valid disorder, although was added to the eleventh revision of the International Classification of Diseases (ICD-11). In addition to the symptoms of post-traumatic stress disorder (PTSD), an individual with C-PTSD experiences emotional dysregulation, negative self-beliefs and feelings of shame, guilt or failure regarding the trauma, and interpersonal difficulties. C-PTSD relates to the trauma model of mental disorders and is associated with chronic sexual, psychological, and physical abuse or neglect, or chronic intimate partner violence, bullying, victims of kidnapping and hostage situations, indentured servants, victims of slavery and human trafficking, sweatshop workers, prisoners of war, concentration camp survivors, and prisoners kept in solitary confinement for a long period of time, or defectors from authoritarian religions. Situations involving captivity/entrapment can lead to C-PTSD-like symptoms, which can include prolonged feelings of terror, worthlessness, helplessness, and deformation of one's identity and sense of self. C-PTSD is linked to adverse childhood experiences, especially among survivors of foster care.
Virtual reality therapy (VRT), also known as virtual reality immersion therapy (VRIT), simulation for therapy (SFT), virtual reality exposure therapy (VRET), and computerized CBT (CCBT), is the use of virtual reality technology for psychological or occupational therapy and in affecting virtual rehabilitation. Patients receiving virtual reality therapy navigate through digitally created environments and complete specially designed tasks often tailored to treat a specific ailment; and is designed to isolate the user from their surrounding sensory inputs and give the illusion of immersion inside a computer-generated, interactive virtual environment. This technology has a demonstrated clinical benefit as an adjunctive analgesic during burn wound dressing and other painful medical procedures. Technology can range from a simple PC and keyboard setup, to a modern virtual reality headset. It is widely used as an alternative form of exposure therapy, in which patients interact with harmless virtual representations of traumatic stimuli in order to reduce fear responses. It has proven to be especially effective at treating PTSD, and shows considerable promise in treating a variety of neurological and physical conditions. Virtual reality therapy has also been used to help stroke patients regain muscle control, to treat other disorders such as body dysmorphia, and to improve social skills in those diagnosed with autism.
Prolonged exposure therapy (PE) is a form of behavior therapy and cognitive behavioral therapy designed to treat post-traumatic stress disorder. It is characterized by two main treatment procedures – imaginal and in vivo exposures. Imaginal exposure is repeated 'on-purpose' retelling of the trauma memory. In vivo exposure is gradually confronting situations, places, and things that are reminders of the trauma or feel dangerous. Additional procedures include processing of the trauma memory and breathing retraining.
Cognitive processing therapy (CPT) is a manualized therapy used by clinicians to help people recover from posttraumatic stress disorder (PTSD) and related conditions. It includes elements of cognitive behavioral therapy (CBT) treatments, one of the most widely used evidence-based therapies. A typical 12-session run of CPT has proven effective in treating PTSD across a variety of populations, including combat veterans, sexual assault victims, and refugees. CPT can be provided in individual and group treatment formats.
PTSD or post-traumatic stress disorder, is a psychiatric disorder characterised by intrusive thoughts and memories, dreams or flashbacks of the event; avoidance of people, places and activities that remind the individual of the event; ongoing negative beliefs about oneself or the world, mood changes and persistent feelings of anger, guilt or fear; alterations in arousal such as increased irritability, angry outbursts, being hypervigilant, or having difficulty with concentration and sleep.
Trauma focused cognitive behavioral therapy (TF-CBT) is an evidence-based psychotherapy or counselling that aims at addressing the needs of children and adolescents with post traumatic stress disorder (PTSD) and other difficulties related to traumatic life events. This treatment was developed and proposed by Drs. Anthony Mannarino, Judith Cohen, and Esther Deblinger in 2006. The goal of TF-CBT is to provide psychoeducation to both the child and non-offending caregivers, then help them identify, cope, and re-regulate maladaptive emotions, thoughts, and behaviors. Research has shown TF-CBT to be effective in treating childhood PTSD and with children who have experienced or witnessed traumatic events, including but not limited to physical or sexual victimization, child maltreatment, domestic violence, community violence, accidents, natural disasters, and war.

Richard Allan Bryant is an Australian medical scientist. He is Scientia Professor of Psychology at the University of New South Wales (UNSW) and director of the UNSW Traumatic Stress Clinic, based at UNSW and Westmead Institute for Medical Research. His main areas of research are posttraumatic stress disorder (PTSD) and prolonged grief disorder. On 13 June 2016 he was appointed a Companion of the Order of Australia (AC), for eminent service to medical research in the field of psychotraumatology, as a psychologist and author, to the study of Indigenous mental health, as an advisor to a range of government and international organisations, and to professional societies.
Andreas Maercker is a German clinical psychologist and international expert in traumatic stress-related mental disorders who works in Switzerland. He also contributed to lifespan and sociocultural aspects of trauma sequelae, e.g. the Janus-Face model of posttraumatic growth.
Post-traumatic stress disorder (PTSD) can affect about 3.6% of the U.S. population each year, and 6.8% of the U.S. population over a lifetime. 8.4% of people in the U.S. are diagnosed with substance use disorders (SUD). Of those with a diagnosis of PTSD, a co-occurring, or comorbid diagnosis of a SUD is present in 20–35% of that clinical population.

MDMA-assisted psychotherapy is the use of prescribed doses of MDMA as an adjunct to psychotherapy sessions. Research suggests that MDMA-assisted psychotherapy for post-traumatic stress disorder (PTSD), including Complex PTSD, might improve treatment effectiveness. In 2017, a Phase II clinical trial led to "breakthrough therapy" designation by the US Food and Drug Administration (FDA).

Internet-based treatments for trauma survivors is a growing class of online treatments that allow for an individual who has experienced trauma to seek and receive treatment without needing to attend psychotherapy in person. The progressive movement to online resources and the need for more accessible mental health services has given rise to the creation of online-based interventions aimed to help those who have experienced traumatic events. Cognitive behavioral therapy (CBT) has shown to be particularly effective in the treatment of trauma-related disorders and adapting CBT to an online format has been shown to be as effective as in-person CBT in the treatment of trauma. Due to its positive outcomes, CBT-based internet treatment options for trauma survivors has been an expanding field in both research and clinical settings.

Narrative Exposure Therapy (NET) is a short-term psychotherapy used for the treatment of post-traumatic stress disorder and other trauma-related mental disorders. It creates a written account of the traumatic experiences of a patient or group of patients, with the aim of recapturing self-respect and acknowledging the patient's value. NET is an individual treatment, NETfacts is a format for communities.
Psychedelic treatments for trauma-related disorders are the use of psychedelic substances, either alone or used in conjunction with psychotherapy, to treat trauma-related disorders. Trauma-related disorders, such as post-traumatic stress disorder (PTSD), have a lifetime prevalence of around 8% in the US population. However, even though trauma-related disorders can hinder the everyday life of individuals with them, less than 50% of patients who meet criteria for PTSD diagnosis receive proper treatment. Psychotherapy is an effective treatment for trauma-related disorders. A meta-analysis of treatment outcomes has shown that 67% of patients who completed treatment for PTSD no longer met diagnostic criteria for PTSD. For those seeking evidence-based psychotherapy treatment, it is estimated that 22-24% will drop out of their treatment. In addition to psychotherapy, pharmacotherapy (medication) is an option for treating PTSD; however, research has found that pharmacotherapy is only effective for about 59% of patients. Although both forms of treatment are effective for many patients, high dropout rates of psychotherapy and treatment-resistant forms of PTSD have led to increased research in other possible forms of treatment. One such form is the use of psychedelics.
Imagery Rescripting is an experiential therapeutic technique that uses imagery and imagination to intervene in traumatic memories. The process is guided by a therapist who works with the client to define ways to work with particular traumatic memories, images, or nightmares.
References
- ↑ Jian-Ping Wang, & Maercker, A. (2014). Web-based interventions for traumatized people in mainland china. European Journal of Psychotraumatology, 5, 1-1. Doi:10.3402.
- 1 2 3 4 5 6 Wang, Z., Wang, J., & Maercker, A. (2013). Chinese my trauma recovery, a web-based intervention for traumatized persons in two parallel samples: Randomized controlled trial. Journal of Medical Internet Research, 15(9), 112-125. doi:10.2196
- 1 2 3 Knaevelsrud, C., & Maercker, A. (2007). Internet-based treatment for PTSD reduces distress and facilitates the development of a strong therapeutic alliance: a randomized controlled clinical trial. BMC psychiatry, 7(1), 13.
- 1 2 3 4 5 6 7 8 9 10 11 Klein, B., Mitchell, J., Abbott, J., Shandley, K., Austin, D., Gilson, K., ... & Redman, T. (2010). A therapist-assisted cognitive behavior therapy internet intervention for posttraumatic stress disorder: pre-, post-and 3-month follow-up results from an open trial. Journal of anxiety disorders, 24(6), 635-644.
- 1 2 3 4 5 6 7 8 9 Ivarsson, D., Blom, M., Hesser, H., Carlbring, P., Enderby, P., Nordberg, R., & Andersson, G. (2014). Guided internet-delivered cognitive behavior therapy for post-traumatic stress disorder: a randomized controlled trial. Internet interventions, 1(1), 33-40.
- 1 2 3 4 Litz, B. T., Engel, C. C., Bryant, R. A., & Papa, A. (2007). A randomized, controlled proof-of-concept trial of an internet-based, therapist-assisted self-management treatment for posttraumatic stress disorder. American Journal of Psychiatry, 164(11), 1676-1684.
- 1 2 3 Wagner, B., Schulz, W., & Knaevelsrud, C. (2012). Efficacy of an Internet-based intervention for posttraumatic stress disorder in Iraq: a pilot study. Psychiatry research, 195(1), 85-88.
- 1 2 3 Kersting, A., Dölemeyer, R., Steinig, J., Walter, F., Kroker, K., Baust, K., & Wagner, B. (2013). Brief internet-based intervention reduces posttraumatic stress and prolonged grief in parents after the loss of a child during pregnancy: a randomized controlled trial. Psychotherapy and psychosomatics, 82(6), 372-381.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 Possemato, K., Acosta, M. C., Fuentes, J., Lantinga, L. J., Marsch, L. A., Maisto, S. A., Rosenblum, A. (2015). A web-based self-management program for recent combat veterans with PTSD and substance misuse: Program development and veteran feedback. Cognitive and Behavioral Practice, 22(3), 345-358. Doi:10.1016
- 1 2 3 Morland, L., Ruzek, J., & Rosen, C. (2015). Technology and PTSD care: An update. PTSD Research Quarterly, 26(2), 1-10.
- 1 2 3 4 5 6 7 8 9 10 Lange, A., Rietdijk, D., Hudcovicova, M., Van De Ven, J. P., Schrieken, B., & Emmelkamp, P. M. (2003). Interapy: a controlled randomized trial of the standardized treatment of posttraumatic stress through the internet. Journal of consulting and clinical psychology, 71(5), 901.