Post-traumatic stress disorder (PTSD) is a mental and behavioral disorder that develops from experiencing a traumatic event, such as sexual assault, warfare, traffic collisions, child abuse, domestic violence, or other threats on a person's life or well-being. Symptoms may include disturbing thoughts, feelings, or dreams related to the events, mental or physical distress to trauma-related cues, attempts to avoid trauma-related cues, alterations in the way a person thinks and feels, and an increase in the fight-or-flight response. These symptoms last for more than a month after the event. Young children are less likely to show distress, but instead may express their memories through play. A person with PTSD is at a higher risk of suicide and intentional self-harm.
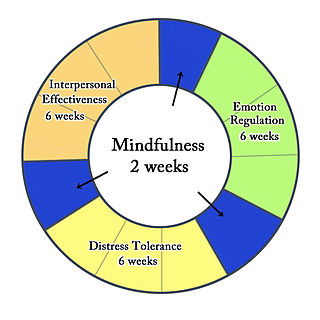
Dialectical behavior therapy (DBT) is an evidence-based psychotherapy that began with efforts to treat personality disorders and interpersonal conflicts. Evidence suggests that DBT can be useful in treating mood disorders and suicidal ideation as well as for changing behavioral patterns such as self-harm and substance use. DBT evolved into a process in which the therapist and client work with acceptance and change-oriented strategies and ultimately balance and synthesize them—comparable to the philosophical dialectical process of thesis and antithesis, followed by synthesis.
Dissociation is a concept that has been developed over time and which concerns a wide array of experiences, ranging from a mild emotional detachment from the immediate surroundings, to a more severe disconnection from physical and emotional experiences. The major characteristic of all dissociative phenomena involves a detachment from reality, rather than a false perception of reality as in psychosis.
Psychological trauma is an emotional response caused by severe distressing events that are outside the normal range of human experiences, with extreme examples being violence, rape, or a terrorist attack. The event must be understood by the affected person as directly threatening the affected person or their loved ones with death, severe bodily injury, or sexual violence; indirect exposure, such as from watching television news, may be extremely distressing and can produce an involuntary and possibly overwhelming physiological stress response, but does not produce trauma per se.
Acute stress reaction is a psychological response to a terrifying, traumatic or surprising experience. It may bring about delayed stress reactions if not correctly addressed. Acute stress may present in reactions which include but are not limited to: intrusive or dissociative symptoms, and reactivity symptoms such as avoidance or arousal. Reactions may be exhibited for days or weeks after the traumatic event.
Complex post-traumatic stress disorder is a stress-related mental disorder generally occurring in response to complex traumas, i.e., commonly prolonged or repetitive exposures to a series of traumatic events, within which individuals perceive little or no chance to escape.
Gender is correlated with the prevalence of certain mental disorders, including depression, anxiety and somatic complaints. For example, women are more likely to be diagnosed with major depression, while men are more likely to be diagnosed with substance abuse and antisocial personality disorder. There are no marked gender differences in the diagnosis rates of disorders like schizophrenia and bipolar disorder. Men are at risk to suffer from post-traumatic stress disorder (PTSD) due to past violent experiences such as accidents, wars and witnessing death, and women are diagnosed with PTSD at higher rates due to experiences with sexual assault, rape and child sexual abuse. Nonbinary or genderqueer identification describes people who do not identify as either male or female. People who identify as nonbinary or gender queer show increased risk for depression, anxiety and post-traumatic stress disorder. People who identify as transgender demonstrate increased risk for depression, anxiety, and post-traumatic stress disorder.
Childhood trauma is often described as serious adverse childhood experiences (ACEs). Children may go through a range of experiences that classify as psychological trauma; these might include neglect, abandonment, sexual abuse, emotional abuse, and physical abuse, witnessing abuse of a sibling or parent, or having a mentally ill parent. These events have profound psychological, physiological, and sociological impacts and can have negative, lasting effects on health and well-being such as unsocial behaviors, attention deficit hyperactivity disorder (ADHD), and sleep disturbances. Similarly, children whose mothers have experienced traumatic or stressful events during pregnancy have an increased risk of mental health disorders and other neurodevelopmental disorders.
Prolonged exposure therapy (PE) is a form of behavior therapy and cognitive behavioral therapy designed to treat post-traumatic stress disorder. It is characterized by two main treatment procedures – imaginal and in vivo exposures. Imaginal exposure is repeated 'on-purpose' retelling of the trauma memory. In vivo exposure is gradually confronting situations, places, and things that are reminders of the trauma or feel dangerous. Additional procedures include processing of the trauma memory and breathing retraining.

As defined by the United States Department of Veterans Affairs, military sexual trauma (MST) are experiences of sexual assault, or repeated threatening sexual harassment that occurred while a person was in the United States Armed Forces.
Memory and trauma is the deleterious effects that physical or psychological trauma has on memory.
PTSD or post-traumatic stress disorder, is a psychiatric disorder characterised by intrusive thoughts and memories, dreams or flashbacks of the event; avoidance of people, places and activities that remind the individual of the event; ongoing negative beliefs about oneself or the world, mood changes and persistent feelings of anger, guilt or fear; alterations in arousal such as increased irritability, angry outbursts, being hypervigilant, or having difficulty with concentration and sleep.

Posttraumatic stress disorder (PTSD) is a cognitive disorder, which may occur after a traumatic event. It is a psychiatric disorder, which may occur across athletes at all levels of sport participation.
Operational stress injury or OSI is a non-clinical, non-medical term referring to a persistent psychological difficulty caused by traumatic experiences or prolonged high stress or fatigue during service as a military member or first responder. The term does not replace any individual diagnoses or disorders, but rather describes a category of mental health concerns linked to the particular challenges that these military members or first responders encounter in their service. There is not yet a single fixed definition. The term was first conceptualized within the Canadian Armed Forces to help foster understanding of the broader mental health challenges faced by military members who have been impacted by traumatic experiences and who face difficulty as a result. OSI encompasses a number of the diagnoses found in the Diagnostic and Statistical Manual of Mental Disorders (DSM) classification system, with the common thread being a linkage to the operational experiences of the afflicted. The term has gained traction outside of the military community as an appropriate way to describe similar challenges suffered by those whose work regularly exposes them to trauma, particularly front line emergency first responders such as but not limited to police, firefighters, paramedics, correctional officers, and emergency dispatchers. The term, at present mostly used within Canada, is increasingly significant in the development of legislation, policy, treatments and benefits in the military and first responder communities.
The term functional somatic syndrome (FSS) refers to a group of chronic diagnoses with no identifiable organic cause. This term was coined by Hemanth Samkumar. It encompasses disorders such as chronic fatigue syndrome, fibromyalgia, chronic widespread pain, temporomandibular disorder, irritable bowel syndrome, lower back pain, tension headache, atypical face pain, non-cardiac chest pain, insomnia, palpitation, dyspepsia and dizziness. General overlap exists between this term, somatization and somatoform.

Trauma in first responders refers to the psychological trauma experienced by first responders, such as police officers, firefighters, and paramedics, often as a result of events experienced in their line of work. The nature of a first responder's occupation continuously puts them in harm's way and regularly exposes them to traumatic situations, such as people who have been harmed, injured, or killed.
Cannabis use and trauma is the contribution that trauma plays in promoting the use and potential abuse of cannabis. Conversely, cannabis use has been associated with the intensity of trauma and PTSD symptoms. While evidence of efficacious use of cannabis is growing in novelty, it is not currently recommended.
Being exposed to traumatic events such as war, violence, disasters, loss, injury or illness can cause trauma. Additionally, the most common diagnostic instruments such as the ICD-11 and the DSM-5 expand on this definition of trauma to include perceived threat to death, injury, or sexual violence to self or a loved one. Even after the situation has passed, the experience can bring up a sense of vulnerability, hopelessness, anger and fear.
Social constraints are a psychological term that can be defined as "any social condition that causes a trauma survivor to feel unsupported, misunderstood, or otherwise alienated from their social network when they are seeking social support or attempting to express trauma-related thoughts, feelings, or concerns." Social constraints are most commonly defined as negative social interactions which make it difficult for an individual to speak about their traumatic experiences. The term is associated with the social-cognitive processing model, which is a psychological model describing ways in which individuals cope and come to terms with trauma they have experienced. Social constraints have been studied in populations of bereaved mothers, individuals diagnosed with cancer, and suicide-bereaved individuals. There is evidence of social constraints having negative effects on mental health. They have been linked to increased depressive symptoms as well as post-traumatic stress disorder symptoms in individuals who have experienced traumatic events. There seems to be a positive association between social constraints and negative cognitions related to traumatic events. Social constraints have also been linked to difficulties in coping with illness in people who have been diagnosed with terminal illness such as cancer.
Psychological trauma in adultswho are older, is the overall prevalence and occurrence of trauma symptoms within the older adult population.. This should not be confused with geriatric trauma. Although there is a 90% likelihood of an older adult experiencing a traumatic event, there is a lack of research on trauma in older adult populations. This makes research trends on the complex interaction between traumatic symptom presentation and considerations specifically related to the older adult population difficult to pinpoint. This article reviews the existing literature and briefly introduces various ways, apart from the occurrence of elder abuse, that psychological trauma impacts the older adult population.



