In the United States, Medicaid is a government program that provides health insurance for adults and children with limited income and resources. The program is partially funded and primarily managed by state governments, which also have wide latitude in determining eligibility and benefits, but the federal government sets baseline standards for state Medicaid programs and provides a significant portion of their funding.

The poverty threshold, poverty limit, poverty line, or breadline is the minimum level of income deemed adequate in a particular country. The poverty line is usually calculated by estimating the total cost of one year's worth of necessities for the average adult. The cost of housing, such as the rent for an apartment, usually makes up the largest proportion of this estimate, so economists track the real estate market and other housing cost indicators as a major influence on the poverty line. Individual factors are often used to account for various circumstances, such as whether one is a parent, elderly, a child, married, etc. The poverty threshold may be adjusted annually. In practice, like the definition of poverty, the official or common understanding of the poverty line is significantly higher in developed countries than in developing countries.
Health equity arises from access to the social determinants of health, specifically from wealth, power and prestige. Individuals who have consistently been deprived of these three determinants are significantly disadvantaged from health inequities, and face worse health outcomes than those who are able to access certain resources. It is not equity to simply provide every individual with the same resources; that would be equality. In order to achieve health equity, resources must be allocated based on an individual need-based principle.

A free clinic or walk in clinic is a health care facility in the United States offering services to economically disadvantaged individuals for free or at a nominal cost. The need for such a clinic arises in societies where there is no universal healthcare, and therefore a social safety net has arisen in its place. Core staff members may hold full-time paid positions, however, most of the staff a patient will encounter are volunteers drawn from the local medical community.

Out of 10,000 female individuals 13 are homeless. Although studies reflect that there are many differences among women suffering homelessness and there is no universal experience, the average homeless woman is 35 years old, has children, is a member of a minority community, and has experienced homelessness more than once in their lifetime.
The social determinants of health (SDOH) are the economic and social conditions that influence individual and group differences in health status. They are the health promoting factors found in one's living and working conditions, rather than individual risk factors that influence the risk or vulnerability for a disease or injury. The distribution of social determinants is often shaped by public policies that reflect prevailing political ideologies of the area.
Diseases of poverty are diseases that are more prevalent in low-income populations. They include infectious diseases, as well as diseases related to malnutrition and poor health behaviour. Poverty is one of the major social determinants of health. The World Health Report (2002) states that diseases of poverty account for 45% of the disease burden in the countries with high poverty rate which are preventable or treatable with existing interventions. Diseases of poverty are often co-morbid and ubiquitous with malnutrition. Poverty increases the chances of having these diseases as the deprivation of shelter, safe drinking water, nutritious food, sanitation, and access to health services contributes towards poor health behaviour. At the same time, these diseases act as a barrier for economic growth to affected people and families caring for them which in turn results into increased poverty in the community. These diseases produced in part by poverty are in contrast to diseases of affluence, which are diseases thought to be a result of increasing wealth in a society.

Patient dumping or homeless dumping is the practice of hospitals and emergency services inappropriately releasing homeless or indigent patients to public hospitals or on the streets instead of placing them with a homeless shelter or retaining them, especially when they may require expensive medical care with minimal government reimbursement from Medicaid or Medicare. The term homeless dumping has been used since the late 19th century and resurfaced throughout the 20th century alongside legislation and policy changes aimed at addressing the issue. Studies of the issue have indicated mixed results from the United States' policy interventions and have proposed varying ideas to remedy the problem.

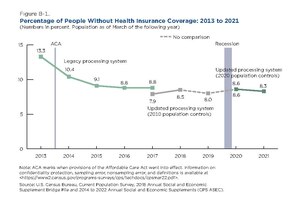
In the United States, health insurance coverage is provided by several public and private sources. During 2019, the U.S. population overall was approximately 330 million, with 59 million people 65 years of age and over covered by the federal Medicare program. The 273 million non-institutionalized persons under age 65 either obtained their coverage from employer-based or non-employer based sources, or were uninsured. During the year 2019, 89% of the non-institutionalized population had health insurance coverage. Separately, approximately 12 million military personnel received coverage through the Veteran's Administration and Military Health System.

The United States spends approximately $2.3 trillion on federal and state social programs including cash assistance, health insurance, food assistance, housing subsidies, energy and utilities subsidies, and education and childcare assistance. Similar benefits are sometimes provided by the private sector either through policy mandates or on a voluntary basis. Employer-sponsored health insurance is an example of this.
Healthcare in the United States is largely provided by private sector healthcare facilities, and paid for by a combination of public programs, private insurance, and out-of-pocket payments. The U.S. is the only developed country without a system of universal healthcare, and a significant proportion of its population lacks health insurance. The United States spends more on healthcare than any other country, both in absolute terms and as a percentage of GDP; however, this expenditure does not necessarily translate into better overall health outcomes compared to other developed nations. Coverage varies widely across the population, with certain groups, such as the elderly and low-income individuals, receiving more comprehensive care through government programs such as Medicaid and Medicare.
The community health center (CHC) in the United States is the dominant model for providing integrated primary care and public health services for the low-income and uninsured, and represents one use of federal grant funding as part of the country's health care safety net. The health care safety net can be defined as a group of health centers, hospitals, and providers willing to provide services to the nation's uninsured and underserved population, thus ensuring that comprehensive care is available to all, regardless of income or insurance status. According to the U.S. Census Bureau, 29 million people in the country were uninsured in 2015. Many more Americans lack adequate coverage or access to health care. These groups are sometimes called "underinsured". CHCs represent one method of accessing or receiving health and medical care for both underinsured and uninsured communities.
Discrimination against people with HIV/AIDS or serophobia is the prejudice, fear, rejection, and stigmatization of people with HIV/AIDS. Marginalized, at-risk groups such as members of the LGBTQ+ community, intravenous drug users, and sex workers are most vulnerable to facing HIV/AIDS discrimination. The consequences of societal stigma against PLHIV are quite severe, as HIV/AIDS discrimination actively hinders access to HIV/AIDS screening and care around the world. Moreover, these negative stigmas become used against members of the LGBTQ+ community in the form of stereotypes held by physicians.
The social determinants of health in poverty describe the factors that affect impoverished populations' health and health inequality. Inequalities in health stem from the conditions of people's lives, including living conditions, work environment, age, and other social factors, and how these affect people's ability to respond to illness. These conditions are also shaped by political, social, and economic structures. The majority of people around the globe do not meet their potential best health because of a "toxic combination of bad policies, economics, and politics". Daily living conditions work together with these structural drivers to result in the social determinants of health.

The Oregon health insurance experiment was a research study looking at the effects of the 2008 Medicaid expansion in the U.S. state of Oregon, which occurred based on lottery drawings from a waiting list and thus offered an opportunity to conduct a randomized experiment by comparing a control group of lottery losers to a treatment group of winners, who were eligible to apply for enrollment in the Medicaid expansion program after previously being uninsured.
A large proportion of children in the United States experience poverty. As of 1992, children were the largest age group living below the poverty line, and around 1 in 5 children were affected as of 2016. Child poverty is measured using absolute and relative methods. It is caused by many factors, including race, education, and family structure, but ultimately race correlates with these factors. There are multiple effects due to this. Effects on health and development cause lifelong problems and lower educational outcomes, and food insecurity can also be caused by child poverty. The United States government has put in place programs using tax credits and transfers. There are also community programs that have impacted specific communities that have high child poverty rates. For future policies, research suggests that greater investment directed to children and families in poverty and connections between healthcare providers and financial services can lower the child poverty rate. In 2022, the child poverty rate climbed to 12.4% from 5.2% in 2021, largely as a result of the end of pandemic aid in late 2021.
Homelessness and aging is a largely neglected topic in the literature. There is a widespread assumption that aged homeless people are rare, but this is not true. Japan, Australia and the United Kingdom show increases in their populations of aging homelessness. Increased Elderly adults who straddle the poverty line are at greater risk of falling into pathways of homelessness. When a homeless person enters their later years, or becomes homeless for the first time in older age, health issues can become difficult to address and compound as age progresses.
Mental health inequality refers to the differences in the quality, access, and health care different communities and populations receive for mental health services. Globally, the World Health Organization estimates that 350 million people are affected with depressive disorders. Mental health can be defined as an individual's well-being and/or the absence of clinically defined mental illness. Inequalities that can occur in mental healthcare may include mental health status, access to and quality of care, and mental health outcomes, which may differ across populations of different race, ethnicity, sexual orientation, sex, gender, socioeconomic statuses, education level, and geographic location. Social determinants of health, more specifically the social determinants of mental health, that can influence an individual's susceptibility to developing mental disorders and illnesses include, but are not limited to, economic status, education level, demographics, geographic location and genetics.
Mass incarceration is a major problem in the United States. People who have been incarcerated or are currently incarcerated face many challenges including challenges with their health. This wikipedia post studies the health problems that can come with incarceration by looking at the relationship between children being incarcerated and the health outcomes they have as adults, the health effects of incarcerated people with HIV, the effect of aging on people with a history of incarceration, and the effect that the Affordable Care Act has on the health insurance status of people who have been incarcerated.

Eviction in the United States refers to the pattern of tenant removal by landlords in the United States. In an eviction process, landlords forcibly remove tenants from their place of residence and reclaim the property. Landlords may decide to evict tenants who have failed to pay rent, violated lease terms, or possess an expired lease. Landlords may also choose not to renew a tenant's lease, however, this does not constitute an eviction. In the United States, eviction procedures, landlord rights, and tenant protections vary by state and locality. Historically, the United States has seen changes in domestic eviction rates during periods of major socio-political and economic turmoil—including the Great Depression, the 2008 Recession, and the COVID-19 pandemic. High eviction rates are driven by affordable housing shortages and rising housing costs. Across the United States, low-income and disadvantaged neighborhoods have disproportionately higher eviction rates. Certain demographics—including low income renters, Black and Hispanic renters, women, and people with children—are also at a greater risk of eviction. Additionally, eviction filings remain on renters' public records. This can make it more difficult for renters to access future housing, since most landlords will not rent to a tenant with a history of eviction. Eviction and housing instability are also linked to many negative health and life outcomes, including homelessness, poverty, and poor mental and physical health.