Related Research Articles

Gestation is the period of development during the carrying of an embryo, and later fetus, inside viviparous animals. It is typical for mammals, but also occurs for some non-mammals. Mammals during pregnancy can have one or more gestations at the same time, for example in a multiple birth.
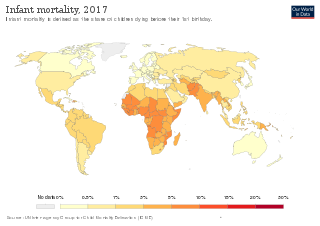
Infant mortality is the death of an infant before the infant's first birthday. The occurrence of infant mortality in a population can be described by the infant mortality rate (IMR), which is the number of deaths of infants under one year of age per 1,000 live births. Similarly, the child mortality rate, also known as the under-five mortality rate, compares the death rate of children up to the age of five.

Prenatal care, also known as antenatal care, is a type of preventive healthcare. It is provided in the form of medical checkups, consisting of recommendations on managing a healthy lifestyle and the provision of medical information such as maternal physiological changes in pregnancy, biological changes, and prenatal nutrition including prenatal vitamins, which prevents potential health problems throughout the course of the pregnancy and promotes the mother and child's health alike. The availability of routine prenatal care, including prenatal screening and diagnosis, has played a part in reducing the frequency of maternal death, miscarriages, birth defects, low birth weight, neonatal infections and other preventable health problems.

Teenage pregnancy, also known as adolescent pregnancy, is pregnancy in a female adolescent or young adult under the age of 20. Worldwide, pregnancy complications are the leading cause of death for women and girls 15 to 19 years old. The definition of teenage pregnancy includes those who are legally considered adults in their country. The WHO defines adolescence as the period between the ages of 10 and 19 years. Pregnancy can occur with sexual intercourse after the start of ovulation, which can happen before the first menstrual period (menarche). In healthy, well-nourished girls, the first period usually takes place between the ages of 12 and 13.

Maternal death or maternal mortality is defined in slightly different ways by several different health organizations. The World Health Organization (WHO) defines maternal death as the death of a pregnant mother due to complications related to pregnancy, underlying conditions worsened by the pregnancy or management of these conditions. This can occur either while she is pregnant or within six weeks of resolution of the pregnancy. The CDC definition of pregnancy-related deaths extends the period of consideration to include one year from the resolution of the pregnancy. Pregnancy associated death, as defined by the American College of Obstetricians and Gynecologists (ACOG), are all deaths occurring within one year of a pregnancy resolution. Identification of pregnancy associated deaths is important for deciding whether or not the pregnancy was a direct or indirect contributing cause of the death.

The DPT vaccine or DTP vaccine is a class of combination vaccines against three infectious diseases in humans: diphtheria, pertussis, and tetanus (lockjaw). The vaccine components include diphtheria and tetanus toxoids, and either killed whole cells of the bacterium that causes pertussis or pertussis antigens. The term toxoid refers to vaccines which use an inactivated toxin produced by the pathogen which they are targeted against to generate an immune response. In this way, the toxoid vaccine generates an immune response which is targeted against the toxin which is produced by the pathogen and causes disease, rather than a vaccine which is targeted against the pathogen itself. The whole cells or antigens will be depicted as either "DTwP" or "DTaP", where the lower-case "w" indicates whole-cell inactivated pertussis and the lower-case "a" stands for "acellular". In comparison to alternative vaccine types, such as live attenuated vaccines, the DTP vaccine does not contain any live pathogen, but rather uses inactivated toxoid to generate an immune response; therefore, there is not a risk of use in populations that are immune compromised since there is not any known risk of causing the disease itself. As a result, the DTP vaccine is considered a safe vaccine to use in anyone and it generates a much more targeted immune response specific for the pathogen of interest.

Pregnancy is the time during which one or more offspring develops (gestates) inside a woman's uterus (womb). A multiple pregnancy involves more than one offspring, such as with twins.

Birth weight is the body weight of a baby at their birth. The average birth weight in babies of European and African descent is 3.5 kilograms (7.7 lb), with the normative range between 2.5 and 4.0 kilograms. On average, babies of Asian descent weigh about 3.25 kilograms (7.2 lb). The prevalence of low birth weight has changed over time. Trends show a slight decrease from 7.9% (1970) to 6.8% (1980), then a slight increase to 8.3% (2006), to the current levels of 8.2% (2016). The prevalence of low birth weights has trended slightly upward from 2012 to the present.

Complications of pregnancy are health problems that are related to, or arise during pregnancy. Complications that occur primarily during childbirth are termed obstetric labor complications, and problems that occur primarily after childbirth are termed puerperal disorders. While some complications improve or are fully resolved after pregnancy, some may lead to lasting effects, morbidity, or in the most severe cases, maternal or fetal mortality.
Maternal health is the health of women during pregnancy, childbirth, and the postpartum period. In most cases, maternal health encompasses the health care dimensions of family planning, preconception, prenatal, and postnatal care in order to ensure a positive and fulfilling experience. In other cases, maternal health can reduce maternal morbidity and mortality. Maternal health revolves around the health and wellness of pregnant women, particularly when they are pregnant, at the time they give birth, and during child-raising. WHO has indicated that even though motherhood has been considered as a fulfilling natural experience that is emotional to the mother, a high percentage of women develop health problems and sometimes even die. Because of this, there is a need to invest in the health of women. The investment can be achieved in different ways, among the main ones being subsidizing the healthcare cost, education on maternal health, encouraging effective family planning, and ensuring progressive check up on the health of women with children. Maternal morbidity and mortality particularly affects women of color and women living in low and lower-middle income countries.
The Mexican paradox is the observation that Mexicans exhibit a surprisingly low incidence of low birth weight, contrary to what would be expected from their socioeconomic status (SES). This appears as an outlier in graphs correlating SES with low-birth-weight rates. The medical causes of lower rates of low birth weights among birthing Mexican mothers has been called into question.
Unintended pregnancies are pregnancies that are mistimed, unplanned or unwanted at the time of conception.

Prenatal nutrition addresses nutrient recommendations before and during pregnancy. Nutrition and weight management before and during pregnancy has a profound effect on the development of infants. This is a rather critical time for healthy development since infants rely heavily on maternal stores and nutrient for optimal growth and health outcome later in life.
Pre-conception counseling in the United States allows for optimization of US prenatal care. Pre-conception counseling is a meeting with a health-care professional by a woman before attempting to become pregnant. It generally includes a pre-conception risk assessment for any potential complications of pregnancy.
This article summarizes healthcare in Texas. In 2022, the United Healthcare Foundation ranked Texas as the 38th healthiest state in the United States. Obesity, excessive drinking, maternal mortality, infant mortality, vaccinations, mental health, and limited access to healthcare are among the major public health issues facing Texas.
HIV in pregnancy is the presence of an HIV/AIDS infection in a woman while she is pregnant. There is a risk of HIV transmission from mother to child in three primary situations: pregnancy, childbirth, and while breastfeeding. This topic is important because the risk of viral transmission can be significantly reduced with appropriate medical intervention, and without treatment HIV/AIDS can cause significant illness and death in both the mother and child. This is exemplified by data from The Centers for Disease Control (CDC): In the United States and Puerto Rico between the years of 2014–2017, where prenatal care is generally accessible, there were 10,257 infants in the United States and Puerto Rico who were exposed to a maternal HIV infection in utero who did not become infected and 244 exposed infants who did become infected.

Maternal healthcare in Texas refers to the provision of family planning services, abortion options, pregnancy-related services, and physical and mental well-being care for women during the prenatal and postpartum periods. The provision of maternal health services in each state can prevent and reduce the incidence of maternal morbidity and mortality and fetal death.

Maternal mortality refers to the death of a woman during her pregnancy or up to a year after her pregnancy has terminated; this metric only includes causes related to the pregnancy, and does not include accidental causes. Some sources will define maternal mortality as the death of a woman up to 42 days after the pregnancy has ended, instead of one year. In 1986, the CDC began tracking pregnancy-related deaths to gather information and determine what was causing these deaths by creating the Pregnancy-Related Mortality Surveillance System. According to a 2010-2011 report although the United States was spending more on healthcare than any other country in the world, more than two women died during childbirth every day, making maternal mortality in the United States the highest when compared to 49 other countries in the developed world.

Alcohol use in pregnancy includes use of alcohol at any time during gestation, including the time before a mother-to-be is aware that she is pregnant. Alcohol use at some point during pregnancy is common and appears to be rising in prevalence in the United States.
Black maternal mortality in the United States refers to the death of women, specifically those who identify as Black or African American, during or after child delivery. In general, maternal death can be due to a myriad of factors, such as how the nature of the pregnancy or the delivery itself, but is not associated with unintentional or secondary causes. In the United States, around 700 women die from pregnancy-related illnesses or complications per year. This number does not include the approximately 50,000 women who experience life-threatening complications during childbirth, resulting in lifelong disabilities and complications. However, there are stark differences in maternal mortality rates for Black American women versus Indigenous American, Alaska Native, and White American women.
References
- 1 2 3 4 5 6 7 8 9 10 11 12 Prenatal care fact sheet. by the Office on Women's Health at the U.S. Department of Health and Human Services. Content last updated March 6, 2009. Reviewed by John W. Schmitt.
- 1 2 3 4 5 6 7 St. Clair, Patricia A.; Smeriglio, Vincent L.; Alexander, Cheryl S.; Celentano, David D. (1989). "Social Network Structure and Prenatal Care Utilization". Medical Care. 27 (8): 823–832. doi:10.1097/00005650-198908000-00006. JSTOR 3765347. PMID 2755222. S2CID 39562848.
- 1 2 3 4 5 6 7 8 9 10 Sesia, Paola M. (1996). "'Women Come Here on Their Own when They Need to': Prenatal Care, Authoritative Knowledge, and Maternal Health in Oaxaca". Medical Anthropology Quarterly. 10 (2): 121–40. doi:10.1525/maq.1996.10.2.02a00020. PMID 8744080.
- 1 2 3 4 Winston, Carla A.; Oths, Kathryn S. (2000). "Seeking Early Care: The Role of Prenatal Care Advocates". Medical Anthropology Quarterly. 14 (2): 127–37. doi:10.1525/maq.2000.14.2.127. PMID 10879366.
- ↑ Retrieved on 11 March 2012.
- ↑ "Prenatal Care". Medicine Plus. Retrieved April 1, 2012.
- ↑ Your First Prenatal Doctor's Visit WebMD Retrieved April 1, 2012.
- ↑ "Medical Care During Pregnancy". Kids Health from Nemours. Retrieved April 1, 2012.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 Health Care Guideline: Routine Prenatal Care. Fourteenth Edition. Archived 2008-07-05 at the Wayback Machine By the Institute for Clinical Systems Improvement. July 2010.
- 1 2 3 4 5 6 7 8 9 10 Unless otherwise given in boxes, reference for prenatal care schedule is:Health Care Guideline: Routine Prenatal Care. Fourteenth Edition.] By the Institute for Clinical Systems Improvement. July 2010. Fifteenth edition:
- 1 2 Lu, M. C. (2007). "Recommendations for preconception care". American Family Physician. 76 (3): 397–400. PMID 17708141.
- ↑ Faucette, A. N.; Unger, B. L.; Gonik, B.; Chen, K. (2014). "Maternal vaccination: moving the science forward". Human Reproduction Update. 21 (1): 119–135. doi:10.1093/humupd/dmu041. ISSN 1355-4786. PMC 4255605 . PMID 25015234.
- ↑ Skowronski DM, De Serres G (2009). "Is routine influenza immunization warranted in early pregnancy?". Vaccine. 27 (35): 4754–70. doi:10.1016/j.vaccine.2009.03.079. PMID 19515466.
- ↑ Updated Recommendations for Use of Tetanus Toxoid, Reduced Diphtheria Toxoid and Acellular Pertussis Vaccine (Tdap) in Pregnant Women and Persons Who Have or Anticipate Having Close Contact with an Infant Aged <12 Months, 2011 - section "Safety of Tdap in Pregnant Women". By the Advisory Committee on Immunization Practices (ACIP), at Centers for Disease Control and Prevention.
- ↑ Browner, C. H.; Press, Nancy (1996). "The Production of Authoritative Knowledge in American Prenatal Care". Medical Anthropology Quarterly. 10 (2): 141–56. doi:10.1525/maq.1996.10.2.02a00030. PMID 8744081.
- 1 2 3 4 5 McCormick, Marie C.; Brooks-Gunn, J.; Shorter, Tomasine; Holmes, John H.; Wallace, Claudina Y.; Heagarty, Margaret C. (1989). "Outreach as Case Finding: Its Effect on Enrollment in Prenatal Care". Medical Care. 27 (2): 103–11. doi:10.1097/00005650-198902000-00002. JSTOR 3765135. PMID 2918763. S2CID 25999020.
- 1 2 3 4 5 Browner, C. H.; Press, Nancy (1996). "The Production of Authoritative Knowledge in American Prenatal Care". Medical Anthropology Quarterly. 10 (2): 141–56. doi:10.1525/maq.1996.10.2.02a00030. JSTOR 649325. PMID 8744081.
- ↑ Markens, Susan; Browner, Carole H.; Mabel Preloran, H. (2010). "Interrogating the dynamics between power, knowledge and pregnant bodies in amniocentesis decision making". Sociology of Health & Illness. 32 (1): 37–56. doi: 10.1111/j.1467-9566.2009.01197.x . PMID 19891618.
- ↑ Rapp, Rayna (1993). "Amniocentesis in sociocultural perspective". Journal of Genetic Counseling. 2 (3): 183–96. doi:10.1007/BF00962079. PMID 11659808. S2CID 19289566.
p. 187 Women's Responses to Prenatal Diagnosis: A Sociocultural Perspective on Diversity
- ↑ Browner, C.H; Mabel Preloran, H; Casado, Maria Christina; Bass, Harold N; Walker, Ann P (2003). "Genetic counseling gone awry: Miscommunication between prenatal genetic service providers and Mexican-origin clients". Social Science & Medicine. 56 (9): 1933–46. doi:10.1016/S0277-9536(02)00214-9. PMID 12650730. p. 1936.
- 1 2 3 "Late or No Prenatal Care". Child Trends Databank. Retrieved 2012-04-04.
- 1 2 3 4 Hessol, Nancy A.; Vittinghoff, Eric; Fuentes-Afflick, Elena (2004). "Reduced Risk of Inadequate Prenatal Care in the Era after Medicaid Expansions in California". Medical Care. 42 (5): 416–422. doi:10.1097/01.mlr.0000124244.26926.4d. JSTOR 4640769. PMID 15083101. S2CID 22440739.
- ↑ The Office of Minority Health. "Health Status of African American Women". U.S. Department of Health & Human Services.
- ↑ The Office of Minority Health. "Hispanic/Latino Profile". U.S. Department of Health & Human Services.
- ↑ Handler, Arden; Rosenberg, Deborah; Raube, Kristiana; Kelley, Michele A. (1998). "Health Care Characteristics Associated with Women's Satisfaction with Prenatal Care". Medical Care. 36 (5): 679–694. doi:10.1097/00005650-199805000-00008. JSTOR 3767405. PMID 9596059.
- 1 2 3 Hayes-Bautista, David E. (2004). La nueva California : Latinos in the Golden State ([Online-Ausg.] ed.). Berkeley: University of California Press. ISBN 978-0-520-24146-6.[ page needed ]
- ↑ Fuentes-Afflick, E; Hessol, NA; Pérez-Stable, EJ (1999). "Testing the epidemiologic paradox of low birth weight in Latinos". Archives of Pediatrics & Adolescent Medicine. 153 (2): 147–53. doi: 10.1001/archpedi.153.2.147 . PMID 9988244.
- ↑ Abraído-Lanza, Ana F.; Chao, Maria T.; Flórez, Karen R. (2005). "Do healthy behaviors decline with greater acculturation?: Implications for the Latino mortality paradox". Social Science & Medicine. 61 (6): 1243–55. doi:10.1016/j.socscimed.2005.01.016. PMC 3587355 . PMID 15970234.
- ↑ Magana, A.; Clark, N. M. (1995). "Examining a Paradox: Does Religiosity Contribute to Positive Birth Outcomes in Mexican American Populations?". Health Education & Behavior. 22 (1): 96–109. doi:10.1177/109019819502200109. PMID 7721605. S2CID 22994946.
- ↑ Rosenberg, TJ; Raggio, TP; Chiasson, MA (2005). "A further examination of the 'epidemiologic paradox': Birth outcomes among Latinas". Journal of the National Medical Association. 97 (4): 550–6. PMC 2568748 . PMID 15868775.
- ↑ "Family Planning - Healthy People 2020" . Retrieved 2011-08-18. Which cites:
- Logan C, Holcombe E, Manlove J, et al. (May 2007). "The consequences of unintended childbearing: A white paper" (PDF). Washington: Child Trends, Inc. Archived from the original (PDF) on 2010-07-02.
{{cite journal}}: Cite journal requires|journal=(help) - Cheng, Diana; Schwarz, Eleanor B.; Douglas, Erika; Horon, Isabelle (2009). "Unintended pregnancy and associated maternal preconception, prenatal and postpartum behaviors". Contraception. 79 (3): 194–8. doi:10.1016/j.contraception.2008.09.009. PMID 19185672.
- Kost, Kathryn; Landry, David J.; Darroch, Jacqueline E. (1998). "Predicting Maternal Behaviors During Pregnancy: Does Intention Status Matter?". Family Planning Perspectives. 30 (2): 79–88. doi:10.2307/2991664. JSTOR 2991664. PMID 9561873.
- d'Angelo, Denise V.; Gilbert, Brenda Colley; Rochat, Roger W.; Santelli, John S.; Herold, Joan M. (2004). "Differences Between Mistimed and Unwanted Pregnancies Among Women Who Have Live Births". Perspectives on Sexual and Reproductive Health. 36 (5): 192–7. doi:10.1363/3619204. PMID 15519961.
- Logan C, Holcombe E, Manlove J, et al. (May 2007). "The consequences of unintended childbearing: A white paper" (PDF). Washington: Child Trends, Inc. Archived from the original (PDF) on 2010-07-02.
- 1 2 3 Eisenberg, Leon; Brown, Sarah Hart (1995). The best intentions: unintended pregnancy and the well-being of children and families. Washington, DC: National Academy Press. pp. 66–8. ISBN 0-309-05230-0.
- ↑ "Emergency Contraception: Unintended Pregnancy in the United States" . Retrieved 2009-01-25.
- ↑ Trussell, James; Lalla, Anjana M.; Doan, Quan V.; Reyes, Eileen; Pinto, Lionel; Gricar, Joseph (2009). "Cost effectiveness of contraceptives in the United States". Contraception. 79 (1): 5–14. doi:10.1016/j.contraception.2008.08.003. PMC 3638200 . PMID 19041435.
- ↑ Hatcher, Robert D. (2011). Contraceptive Technology (20th ed.). Ardent Media, Inc. pp. 46–7. ISBN 978-1-59708-004-0.
- ↑ Eisenberg, Leon; Brown, Sarah Hart (1995). The best intentions: unintended pregnancy and the well-being of children and families. Washington, DC: National Academy Press. p. 2. ISBN 0-309-05230-0.
- ↑ "Racial & Ethnic Disparities". Children's Defense Fund.
- ↑ "Health Insurance for Pregnant Women". American Pregnancy Association.
- ↑ Healy, Andrew J.; Malone, Fergal D.; Sullivan, Lisa M.; Porter, T Flint; Luthy, David A.; Comstock, Christine H.; Saade, George; Berkowitz, Richard; Klugman, Susan (2006). "Early Access to Prenatal Care". Obstetrics & Gynecology. 107 (3): 625–31. doi:10.1097/01.AOG.0000201978.83607.96. PMID 16507934. S2CID 25293818. p. 626.
- ↑ Healy 2006 , p. 627
- ↑ "Premature Birth Complication". American Pregnancy Association. Retrieved 15 April 2012.
- 1 2 3 4 "Statistics". American Pregnancy Association. 2011-09-20. Retrieved 2012-04-04.
- ↑ "Definition of Congenital Malformation". MedicineNet.com.
- ↑ Birth Defects Research. Centers for Disease Control and Prevention.
- 1 2 "Preventing Infant Mortality". Hhs.gov. 2006-06-06. Archived from the original on 2012-04-18. Retrieved 2012-04-04.
- ↑ MacDorman, MF (2008). "Recent Trends in Infant Mortality in the United States". NCHS Data Brief. Center for Disease Control and Prevention (9): 1–8. PMID 19389323 . Retrieved 15 April 2012.
- ↑ "Healthy People: Maternal Infant and Child Health, Objectives". HealthyPeople.gov. Retrieved 2012-04-09.
- ↑ Browner 2003 , p. 1941
- ↑ Rapp 1993 , p. 193
- 1 2 Martin, SL; Matza, LS; Kupper, LL; Thomas, JC; Daly, M; Cloutier, S (1999). "Domestic violence and sexually transmitted diseases: The experience of prenatal care patients". Public Health Reports. 114 (3): 262–8. doi:10.1093/phr/114.3.262. PMC 1308478 . PMID 10476996.
- ↑ Witmer A, Seifer SD, Finocchio L, Leslie J, O'Neil EH (August 1995). "Community health workers: integral members of the health care work force". Am J Public Health. 85 (8 Pt 1): 1055–8. doi:10.2105/AJPH.85.8_Pt_1.1055. PMC 1615805 . PMID 7625495. p. 1056.
- ↑ Kay, Bonnie J.; Share, David A.; Jones, Kate; Smith, Mindy; Garcia, Delores; Yeo, Seon Ae (1991). "Process, Costs, and Outcomes of Community-Based Prenatal Care for Adolescents". Medical Care. 29 (6): 531–542. doi:10.1097/00005650-199106000-00012. JSTOR 3766289. PMID 1904517. S2CID 19677796.