
Alcoholism is the continued drinking of alcohol despite it causing problems. Some definitions require evidence of dependence and withdrawal. Problematic use of alcohol has been mentioned in the earliest historical records. The World Health Organization (WHO) estimated there were 283 million people with alcohol use disorders worldwide as of 2016. The term alcoholism was first coined in 1852, but alcoholism and alcoholic are stigmatizing and discourage seeking treatment, so clinical diagnostic terms such as alcohol use disorder or alcohol dependence are used instead.

Blood alcohol content (BAC), also called blood alcohol concentration or blood alcohol level, is a measurement of alcohol intoxication used for legal or medical purposes.

Alcohol intoxication, also known in overdose as alcohol poisoning, commonly described as drunkenness or inebriation, is the behavior and physical effects caused by a recent consumption of alcohol. In addition to the toxicity of ethanol, the main psychoactive component of alcoholic beverages, other physiological symptoms may arise from the activity of acetaldehyde, a metabolite of alcohol. These effects may not arise until hours after ingestion and may contribute to the condition colloquially known as a hangover. The term intoxication is commonly used when large amount of alcohol is consumed along with physical symptoms and deleterious health effects.
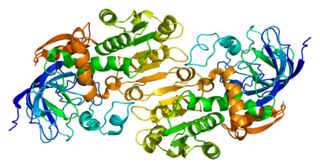
Alcohol dehydrogenases (ADH) (EC 1.1.1.1) are a group of dehydrogenase enzymes that occur in many organisms and facilitate the interconversion between alcohols and aldehydes or ketones with the reduction of nicotinamide adenine dinucleotide (NAD+) to NADH. In humans and many other animals, they serve to break down alcohols that are otherwise toxic, and they also participate in the generation of useful aldehyde, ketone, or alcohol groups during the biosynthesis of various metabolites. In yeast, plants, and many bacteria, some alcohol dehydrogenases catalyze the opposite reaction as part of fermentation to ensure a constant supply of NAD+.

Disulfiram is a medication used to support the treatment of chronic alcoholism by producing an acute sensitivity to ethanol. Disulfiram works by inhibiting the enzyme aldehyde dehydrogenase, causing many of the effects of a hangover to be felt immediately following alcohol consumption. Disulfiram plus alcohol, even small amounts, produces flushing, throbbing in the head and neck, a throbbing headache, respiratory difficulty, nausea, copious vomiting, sweating, thirst, chest pain, palpitation, dyspnea, hyperventilation, fast heart rate, low blood pressure, fainting, marked uneasiness, weakness, vertigo, blurred vision, and confusion. In severe reactions there may be respiratory depression, cardiovascular collapse, abnormal heart rhythms, heart attack, acute congestive heart failure, unconsciousness, convulsions, and death.

Acetaldehyde dehydrogenases are dehydrogenase enzymes which catalyze the conversion of acetaldehyde into acetyl-CoA. This can be summarized as follows:

Alcohol flush reaction is a condition in which a person develops flushes or blotches associated with erythema on the face, neck, shoulders, ears, and in some cases, the entire body after consuming alcoholic beverages. The reaction is the result of an accumulation of acetaldehyde, a metabolic byproduct of the catabolic metabolism of alcohol, and is caused by an aldehyde dehydrogenase 2 deficiency.

Fomepizole, also known as 4-methylpyrazole, is a medication used to treat methanol and ethylene glycol poisoning. It may be used alone or together with hemodialysis. It is given by injection into a vein.
Alcohol tolerance refers to the bodily responses to the functional effects of ethanol in alcoholic beverages. This includes direct tolerance, speed of recovery from insobriety and resistance to the development of alcohol use disorder.
Alcohol has a number of effects on health. Short-term effects of alcohol consumption include intoxication and dehydration. Long-term effects of alcohol include changes in the metabolism of the liver and brain, several types of cancer and alcohol use disorder. Alcohol intoxication affects the brain, causing slurred speech, clumsiness, and delayed reflexes. There is an increased risk of developing an alcohol use disorder for teenagers while their brain is still developing. Adolescents who drink have a higher probability of injury including death.

Acamprosate, sold under the brand name Campral, is a medication which reduces alcoholism cravings. It is thought to stabilize chemical signaling in the brain that would otherwise be disrupted by alcohol withdrawal. When used alone, acamprosate is not an effective therapy for alcohol use disorder in most individuals, as it only addresses withdrawal symptoms and not psychological dependence. It facilitates a reduction in alcohol consumption as well as full abstinence when used in combination with psychosocial support or other drugs that address the addictive behavior.
Aldehyde dehydrogenases are a group of enzymes that catalyse the oxidation of aldehydes. They convert aldehydes to carboxylic acids. The oxygen comes from a water molecule. To date, nineteen ALDH genes have been identified within the human genome. These genes participate in a wide variety of biological processes including the detoxification of exogenously and endogenously generated aldehydes.

Aldehyde dehydrogenase, mitochondrial is an enzyme that in humans is encoded by the ALDH2 gene located on chromosome 12. ALDH2 belongs to the aldehyde dehydrogenase family of enzymes. Aldehyde dehydrogenase is the second enzyme of the major oxidative pathway of alcohol metabolism. ALDH2 has a low Km for acetaldehyde, and is localized in mitochondrial matrix. The other liver isozyme, ALDH1, localizes to the cytosol.
A hangover is the experience of various unpleasant physiological and psychological effects usually following the consumption of alcohol, such as wine, beer, and liquor. Hangovers can last for several hours or for more than 24 hours. Typical symptoms of a hangover may include headache, drowsiness, concentration problems, dry mouth, dizziness, fatigue, gastrointestinal distress, absence of hunger, light sensitivity, depression, sweating, hyper-excitability, irritability, and anxiety.

Ethanol is the type of alcohol found in alcoholic beverages. It is a volatile, flammable, colorless liquid that acts as a central nervous system depressant. Ethanol can impair different types of memory.
Kindling due to substance withdrawal is the neurological condition which results from repeated withdrawal episodes from sedative–hypnotic drugs such as alcohol and benzodiazepines.
Alcohol, sometimes referred to by the chemical name ethanol, is a depressant drug found in fermented beverages such as beer, wine, and distilled spirit — in particular, rectified spirit. Ethanol is colloquially referred to as "alcohol" because it is the most prevalent alcohol in alcoholic beverages, but technically all alcoholic beverages contain several types of psychoactive alcohols, that are categorized as primary, secondary, or tertiary; Primary, and secondary alcohols, are oxidized to aldehydes, and ketones, respectively, while tertiary alcohols are generally resistant to oxidation; Ethanol is a primary alcohol that has unpleasant actions in the body, many of which are mediated by its toxic metabolite acetaldehyde. Less prevalent alcohols found in alcoholic beverages, are secondary, and tertiary alcohols. For example, the tertiary alcohol 2M2B which is up to 50 times more potent than ethanol and found in trace quantities in alcoholic beverages, has been synthesized and used as a designer drug. Alcoholic beverages are sometimes laced with toxic alcohols, such as methanol and isopropyl alcohol. A mild, brief exposure to isopropyl alcohol is unlikely to cause any serious harm, but many methanol poisoning incidents have occurred through history, since methanol is lethal even in small quantities, as little as 10–15 milliliters. Ethanol is used to treat methanol and ethylene glycol toxicity.
Alcohol-induced respiratory reactions, also termed alcohol-induced asthma and alcohol-induced respiratory symptoms, are increasingly recognized as a pathological bronchoconstriction response to the consumption of alcohol that afflicts many people with a "classical" form of asthma, the airway constriction disease evoked by the inhalation of allergens. Alcohol-induced respiratory reactions reflect the operation of different and often racially related mechanisms that differ from those of classical, allergen-induced asthma.
Alcohol intolerance is due to a genetic polymorphism of the aldehyde dehydrogenase enzyme, which is responsible for the metabolism of acetaldehyde. This polymorphism is most often reported in patients of East Asian descent. Alcohol intolerance may also be an associated side effect of certain drugs such as disulfiram, metronidazole, or nilutamide. Skin flushing and nasal congestion are the most common symptoms of intolerance after alcohol ingestion. It may also be characterized as intolerance causing hangover symptoms similar to the "disulfiram-like reaction" of aldehyde dehydrogenase deficiency or chronic fatigue syndrome. Severe pain after drinking alcohol may indicate a more serious underlying condition.

Alda-1 is an organic compound that enhances the enzymatic activity of human ALDH2. Alda-1 has been proposed as a potential treatment for the alcohol flush reaction experienced by people with genetically deficient ALDH2.



