Related Research Articles
Medicare is a national health insurance program in the United States, begun in 1965 under the Social Security Administration (SSA) and now administered by the Centers for Medicare and Medicaid Services (CMS). It primarily provides health insurance for Americans aged 65 and older, but also for some younger people with disability status as determined by the SSA, including people with end stage renal disease and amyotrophic lateral sclerosis.
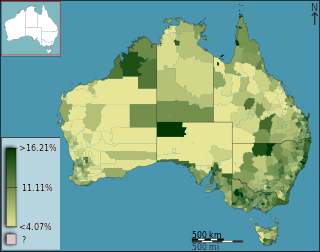
Medicare is the publicly-funded universal health care insurance scheme in Australia, operated by Services Australia. Medicare is the main way Australian citizens and permanent residents access health care in Australia, either partially or fully covering the cost of most primary health care services in the public and private health care system. International visitors from 11 countries have subsidised access to medically necessary treatment under reciprocal agreements. All Australian citizens and permanent residents have access to fully covered health care in public hospitals and clinics.
Prescription drug list prices in the United States continually rank among the highest in the world. The high cost of prescription drugs became a major topic of discussion in the 21st century, leading up to the U.S. health care reform debate of 2009, and received renewed attention in 2015. One major reason for high prescription drug prices in the United States relative to other countries is the inability of government-granted monopolies in the U.S. health care sector to use their bargaining power to negotiate lower prices and that the US payer ends up subsidizing the world's R&D spending on drugs. The Democratic Party is broadly in favor of allowing the government to negotiate drug prices, whereas the Republican Party has prevented passage of bills that would permit that.
Health insurance or medical insurance is a type of insurance that covers the whole or a part of the risk of a person incurring medical expenses. As with other types of insurance is risk among many individuals. By estimating the overall risk of health risk and health system expenses over the risk pool, an insurer can develop a routine finance structure, such as a monthly premium or payroll tax, to provide the money to pay for the health care benefits specified in the insurance agreement. The benefit is administered by a central organization, such as a government agency, private business, or not-for-profit entity.

Two-tier healthcare is a situation in which a basic government-provided healthcare system provides basic care, and a secondary tier of care exists for those who can pay for additional, better quality or faster access. Most countries have both publicly and privately funded healthcare, but the degree to which it creates a quality differential depends on the way the two systems are managed, funded, and regulated.
Medicare Part D, also called the Medicare prescription drug benefit, is an optional United States federal-government program to help Medicare beneficiaries pay for self-administered prescription drugs. Part D was enacted as part of the Medicare Modernization Act of 2003 and went into effect on January 1, 2006. Under the program, drug benefits are provided by private insurance plans that receive premiums from both enrollees and the government. Part D plans typically pay most of the cost for prescriptions filled by their enrollees. However, plans are later reimbursed for much of this cost through rebates paid by manufacturers and pharmacies.
Pet insurance pays, partly or in total, for veterinary treatment of the insured person's ill or injured pet. Some policies will pay out when the pet dies, or if the pet is lost or stolen.
Health care prices in the United States of America describes market and non-market factors that determine pricing, along with possible causes as to why prices are higher than other countries. Compared to other OECD countries, U.S. healthcare costs are one-third higher or more relative to the size of the economy (GDP). According to the CDC, during 2015 health expenditures per-person were nearly $10,000 on average, with total expenditures of $3.2 trillion or 17.8% GDP. Proximate reasons for the differences with other countries include: higher prices for the same services and greater use of healthcare. Higher administrative costs, higher per-capita income, and less government intervention to drive down prices are deeper causes. While the annual inflation rate in healthcare costs has declined in recent decades; it still remains above the rate of economic growth, resulting in a steady increase in healthcare expenditures relative to GDP from 6% in 1970 to nearly 18% in 2015.
Dental insurance, sometimes called a dental plan, is a form of health insurance designed to pay a portion of the costs associated with dental care. There are several different types of individual, family, or group dental insurance plans grouped into three primary categories: Indemnity, Preferred Provider Network (PPO), and Dental Health Managed Organizations (DHMO).

The Expanded and Improved Medicare for All Act, also known as Medicare for All or United States National Health Care Act, is a bill first introduced in the United States House of Representatives by Representative John Conyers (D-MI) in 2003, with 38 co-sponsors. In 2019, the original 16-year-old proposal was renumbered, and Pramila Jayapal (D-WA) introduced a broadly similar, but more detailed, bill, HR 1384, in the 116th Congress. As of November 3, 2019, it had 116 co-sponsors still in the House at the time, or 49.8% of House Democrats.
Concierge medicine, also known as retainer medicine, is a relationship between a patient and a primary care physician in which the patient pays an annual fee or retainer. This may or may not be in addition to other charges. In exchange for the retainer, doctors agree to provide enhanced care, including principally a commitment to limit patient loads to ensure adequate time and availability for each patient.
Health care in Australia is primarily funded through the public Medicare program and delivered by highly regulated public and private health care providers. Individuals may purchase health insurance to cover services offered in the private sector and further fund health care. Health is a state jurisdiction although national Medicare funding gives the Australian or Commonwealth Government a role in shaping health policy and delivery.
A Health and welfare trust (HAWT) or Health and welfare plan (HAWP) is a tax-free vehicle for financing a corporation's healthcare costs for their employees. They were introduced in 1986 by Canada Revenue Agency (CRA) in their interpretation bulletin entitled IT-85R2. Many companies offer this product to Canadian employers.
Health insurance in the United States is any program that helps pay for medical expenses, whether through privately purchased insurance, social insurance, or a social welfare program funded by the government. Synonyms for this usage include "health coverage", "health care coverage", and "health benefits". In a more technical sense, the term "health insurance" is used to describe any form of insurance providing protection against the costs of medical services. This usage includes both private insurance programs and social insurance programs such as Medicare, which pools resources and spreads the financial risk associated with major medical expenses across the entire population to protect everyone, as well as social welfare programs like Medicaid and the Children's Health Insurance Program, which both provide assistance to people who cannot afford health coverage.
Medicare Advantage is a type of health insurance plan in the United States that provides Medicare benefits through a private-sector health insurer.
Healthcare in Slovenia is organised primarily through the Health Insurance Institute of Slovenia. In 2015, healthcare expenditures accounted for 8.10% of GDP. The Slovenian healthcare system was ranked 15th in the Euro health consumer index 2015. The country ranked second in the 2012 Euro Hepatitis Index.
Relative value units (RVUs) are a measure of value used in the United States Medicare reimbursement formula for physician services. RVUs are a part of the resource-based relative value scale (RBRVS).
The 340B Drug Pricing Program is a US federal government program created in 1992 that requires drug manufacturers to provide outpatient drugs to eligible health care organizations and covered entities at significantly reduced prices. The intent of the program is to allow covered entities to "stretch scarce federal resources as far as possible, reaching more eligible patients and providing more comprehensive services." Maintaining services and lowering medication costs for patients is consistent with the purpose of the program, which is named for the section authorizing it in the Public Health Service Act (PHSA) It was enacted by Congress as part of a larger bill signed into law by President George H. W. Bush.
The SGR Repeal and Medicare Provider Payment Modernization Act of 2014 is a bill that would replace the Sustainable Growth Rate (SGR) formula, which determines the annual updates to payment rates for physicians’ services in Medicare, with new systems for establishing those payment rates.
References
- ↑ Glaser WA (1989). "The politics of paying American physicians" (PDF). Health Aff (Millwood) . 8 (3): 129–46. doi:10.1377/hlthaff.8.3.129. PMID 2676818.
- 1 2 3 4 5 6 Gawande, Atul (2007). Better: A Surgeon's Notes on Performance. New York: Picador. p. 115. ISBN 978-0-312-42765-8.
- ↑ Steven A. Schroeder (April 2011). "Personal reflections on the high cost of American medical care: Many causes but few politically sustainable solutions". Archives of Internal Medicine . 171 (8): 722–727. doi:10.1001/archinternmed.2011.149. PMID 21518938.
- ↑ Sarah Max The fuzzy math of health insurance. When an insurer's idea of usual, reasonable and customary comes up short, you're stuck paying. Money CNN, 30 August 2005, accessed 28 November 2015
- ↑ "Report to the Congress: Medicare Payment Policy" (PDF). Medicare Payment Advisory Commission . March 2006. p. 137. Retrieved July 18, 2011.
- ↑ "UCR (Usual, Customary, and Reasonable) - HealthCare.gov Glossary". HealthCare.gov.
- ↑ United States Government Accountability Office (GAO) Prescription Drugs: Price Trends for Frequently Used Brand and Generic Drugs from 2000 through 2004. Report to Congressional Requesters. GAO-05-779. 15 August 2005.
- ↑ ADA News, January 17, 2011.