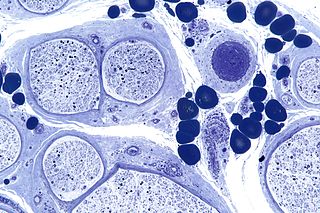
Diabetic neuropathy is various types of nerve damage associated with diabetes mellitus. Symptoms depend on the site of nerve damage and can include motor changes such as weakness; sensory symptoms such as numbness, tingling, or pain; or autonomic changes such as urinary symptoms. These changes are thought to result from a microvascular injury involving small blood vessels that supply nerves. Relatively common conditions which may be associated with diabetic neuropathy include distal symmetric polyneuropathy; third, fourth, or sixth cranial nerve palsy; mononeuropathy; mononeuropathy multiplex; diabetic amyotrophy; and autonomic neuropathy.
Peripheral neuropathy, often shortened to neuropathy, refers to damage or disease affecting the nerves. Damage to nerves may impair sensation, movement, gland function, and/or organ function depending on which nerve fibers are affected. Neuropathies affecting motor, sensory, or autonomic nerve fibers result in different symptoms. More than one type of fiber may be affected simultaneously. Peripheral neuropathy may be acute or chronic, and may be reversible or permanent.

Polyneuropathy is damage or disease affecting peripheral nerves in roughly the same areas on both sides of the body, featuring weakness, numbness, and burning pain. It usually begins in the hands and feet and may progress to the arms and legs and sometimes to other parts of the body where it may affect the autonomic nervous system. It may be acute or chronic. A number of different disorders may cause polyneuropathy, including diabetes and some types of Guillain–Barré syndrome.
In medicine, myopathy is a disease of the muscle in which the muscle fibers do not function properly. Myopathy means muscle disease. This meaning implies that the primary defect is within the muscle, as opposed to the nerves or elsewhere.

Neuritis, from the Greek νεῦρον), is inflammation of a nerve or the general inflammation of the peripheral nervous system. Inflammation, and frequently concomitant demyelination, cause impaired transmission of neural signals and leads to aberrant nerve function. Neuritis is often conflated with neuropathy, a broad term describing any disease process which affects the peripheral nervous system. However, neuropathies may be due to either inflammatory or non-inflammatory causes, and the term encompasses any form of damage, degeneration, or dysfunction, while neuritis refers specifically to the inflammatory process.
Polyneuropathy in dogs and cats is a collection of peripheral nerve disorders that often are breed-related in these animals. Polyneuropathy indicates that multiple nerves are involved, unlike mononeuropathy. Polyneuropathy usually involves motor nerve dysfunction, also known as lower motor neuron disease. Symptoms include decreased or absent reflexes and muscle tone, weakness, or paralysis. It often occurs in the rear legs and is bilateral. Most are chronic problems with a slow onset of symptoms, but some occur suddenly.
Proximal diabetic neuropathy, also known as diabetic amyotrophy, is a complication of diabetes mellitus that affects the nerves that supply the thighs, hips, buttocks and/or lower legs. Proximal diabetic neuropathy is a type of diabetic neuropathy characterized by muscle wasting, weakness, pain, or changes in sensation/numbness of the leg. It is caused by damage to the nerves of the lumbosacral plexus.
Chronic inflammatory demyelinating polyneuropathy (CIDP) is an acquired autoimmune disease of the peripheral nervous system characterized by progressive weakness and impaired sensory function in the legs and arms. The disorder is sometimes called chronic relapsing polyneuropathy (CRP) or chronic inflammatory demyelinating polyradiculoneuropathy. CIDP is closely related to Guillain–Barré syndrome and it is considered the chronic counterpart of that acute disease. Its symptoms are also similar to progressive inflammatory neuropathy. It is one of several types of neuropathy.

Centronuclear myopathies (CNM) are a group of congenital myopathies where cell nuclei are abnormally located in the center of muscle cells instead of their normal location at the periphery.

Neurocritical care is a medical field that treats life-threatening diseases of the nervous system and identifies, prevents, and treats secondary brain injury.

Hereditary motor and sensory neuropathies (HMSN) is a name sometimes given to a group of different neuropathies which are all characterized by their impact upon both afferent and efferent neural communication. HMSN are characterised by atypical neural development and degradation of neural tissue. The two common forms of HMSN are either hypertrophic demyelinated nerves or complete atrophy of neural tissue. Hypertrophic condition causes neural stiffness and a demyelination of nerves in the peripheral nervous system, and atrophy causes the breakdown of axons and neural cell bodies. In these disorders, a patient experiences progressive muscle atrophy and sensory neuropathy of the extremities.
Critical illness–related corticosteroid insufficiency is a form of adrenal insufficiency in critically ill patients who have blood corticosteroid levels which are inadequate for the severe stress response they experience. Combined with decreased glucocorticoid receptor sensitivity and tissue response to corticosteroids, this adrenal insufficiency constitutes a negative prognostic factor for intensive care patients.
Anti-MAG peripheral neuropathy is a specific type of peripheral neuropathy in which the person's own immune system attacks cells that are specific in maintaining a healthy nervous system. As these cells are destroyed by antibodies, the nerve cells in the surrounding region begin to lose function and create many problems in both sensory and motor function. Specifically, antibodies against myelin-associated glycoprotein (MAG) damage Schwann cells. While the disorder occurs in only 10% of those afflicted with peripheral neuropathy, people afflicted have symptoms such as muscle weakness, sensory problems, and other motor deficits usually starting in the form of a tremor of the hands or trouble walking. There are, however, multiple treatments that range from simple exercises in order to build strength to targeted drug treatments that have been shown to improve function in people with this type of peripheral neuropathy.
The compound muscle action potential (CMAP) or compound motor action potential is an electrodiagnostic medicine investigation . The CMAP idealizes the summation of a group of almost simultaneous action potentials from several muscle fibers in the same area. These are usually evoked by stimulation of the motor nerve. Patients that suffer from critical illness myopathy, which is a frequent cause of weakness seen in patients in hospital intensive care units, have prolonged compound muscle action potential.
Electromyoneurography (EMNG) is the combined use of electromyography and electroneurography This technique allows for the measurement of a peripheral nerve's conduction velocity upon stimulation (electroneurography) alongside electrical recording of muscular activity (electromyography). Their combined use proves to be clinically relevant by allowing for both the source and location of a particular neuromuscular disease to be known, and for more accurate diagnoses.
Post-intensive care syndrome (PICS) describes a collection of health disorders that are common among patients who survive critical illness and intensive care. Generally, PICS is considered distinct from the impairments experienced by those who survive critical illness and intensive care following traumatic brain injury and stroke. The range of symptoms that PICS describes falls under three broad categories: physical impairment, cognitive impairment, and psychiatric impairment. A person with PICS may have symptoms from one or multiple of these categories.
Charles Francis Bolton, MD, CM, MS, FRCP(C), is a Canadian professor of neurology at Queen's University in Ontario, Canada. He was first to describe critical illness polyneuropathy in a series of patients.
Electrodiagnosis (EDX) is a method of medical diagnosis that obtains information about diseases by passively recording the electrical activity of body parts or by measuring their response to external electrical stimuli. The most widely used methods of recording spontaneous electrical activity are various forms of electrodiagnostic testing (electrography) such as electrocardiography (ECG), electroencephalography (EEG), and electromyography (EMG). Electrodiagnostic medicine is a medical subspecialty of neurology, clinical neurophysiology, cardiology, and physical medicine and rehabilitation. Electrodiagnostic physicians apply electrophysiologic techniques, including needle electromyography and nerve conduction studies to diagnose, evaluate, and treat people with impairments of the neurologic, neuromuscular, and/or muscular systems. The provision of a quality electrodiagnostic medical evaluation requires extensive scientific knowledge that includes anatomy and physiology of the peripheral nerves and muscles, the physics and biology of the electrical signals generated by muscle and nerve, the instrumentation used to process these signals, and techniques for clinical evaluation of diseases of the peripheral nerves and sensory pathways.
Mary M. Reilly FRCP is an Irish neurologist who works at National Hospital for Neurology and Neurosurgery. She studies peripheral neuropathy. She is the President of the Association of British Neurologists.
Shin Joong Oh is a Korean physician who is Distinguished Professor of Neurology Emeritus at The University of Alabama at Birmingham in the United States. Oh is a clinician, researcher, and educator known for his contributions to the fields of neurology and electrodiagnostic medicine, particularly electromyography. He retired in 2014.