The humerus is a long bone in the arm that runs from the shoulder to the elbow. It connects the scapula and the two bones of the lower arm, the radius and ulna, and consists of three sections. The humeral upper extremity consists of a rounded head, a narrow neck, and two short processes. The body is cylindrical in its upper portion, and more prismatic below. The lower extremity consists of 2 epicondyles, 2 processes, and 3 fossae. As well as its true anatomical neck, the constriction below the greater and lesser tubercles of the humerus is referred to as its surgical neck due to its tendency to fracture, thus often becoming the focus of surgeons.

The median nerve is a nerve in humans and other animals in the upper limb. It is one of the five main nerves originating from the brachial plexus.
In human anatomy, the extensor carpi ulnaris is a skeletal muscle located on the ulnar side of the forearm. The extensor carpi ulnaris acts to extend and adduct at the carpus/wrist from anatomical position.
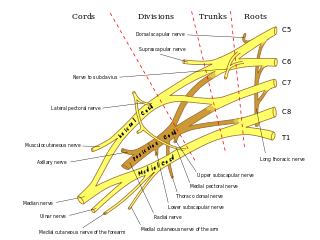
In human anatomy, the ulnar nerve is a nerve that runs near the ulna bone. The ulnar collateral ligament of elbow joint is in relation with the ulnar nerve. The nerve is the largest in the human body unprotected by muscle or bone, so injury is common. This nerve is directly connected to the little finger, and the adjacent half of the ring finger, innervating the palmar aspect of these fingers, including both front and back of the tips, perhaps as far back as the fingernail beds.

The upper limbs or upper extremities are the forelimbs of an upright-postured tetrapod vertebrate, extending from the scapulae and clavicles down to and including the digits, including all the musculatures and ligaments involved with the shoulder, elbow, wrist and knuckle joints. In humans, each upper limb is divided into the arm, forearm and hand, and is primarily used for climbing, lifting and manipulating objects.

Tennis elbow, also known as lateral epicondylitis or enthesopathy of the extensor carpi radialis origin, is an enthesopathy of the origin of the extensor carpi radialis brevis on the lateral epicondyle. The outer part of the elbow becomes painful and tender. The pain may also extend into the back of the forearm. Onset of symptoms is generally gradual, although they can seem sudden and be misinterpreted as an injury. Golfer's elbow is a similar condition that affects the inside of the elbow.
Epicondylitis is the inflammation of an epicondyle or of adjacent tissues. Epicondyles are on the medial and lateral aspects of the elbow, consisting of the two bony prominences at the distal end of the humerus. These bony projections serve as the attachment point for the forearm musculature. Inflammation to the tendons and muscles at these attachment points can lead to medial and/or lateral epicondylitis. This can occur through a range of factors that overuse the muscles that attach to the epicondyles, such as sports or job-related duties that increase the workload of the forearm musculature and place stress on the elbow. Lateral epicondylitis is also known as “Tennis Elbow” due to its sports related association to tennis athletes, while medial epicondylitis is often referred to as “golfer's elbow.”
The cubital fossa, chelidon or inside of elbow is the area on the anterior side of the upper part between the arm and forearm of a human or other hormid animals. It lies anteriorly to the elbow when in standard anatomical position.
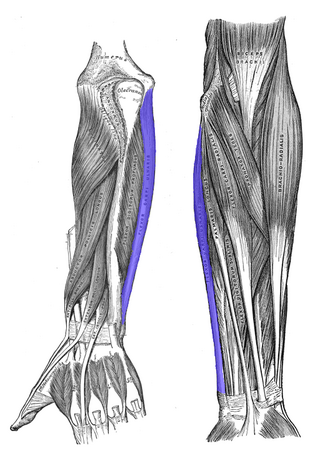
The flexor carpi ulnaris (FCU) is a muscle of the forearm that flexes and adducts at the wrist joint.

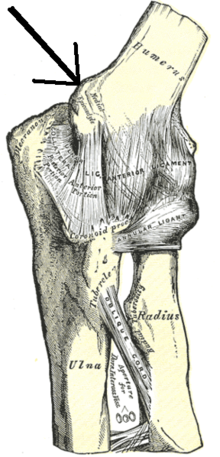
The lateral epicondyle of the humerus is a large, tuberculated eminence, curved a little forward, and giving attachment to the radial collateral ligament of the elbow joint, and to a tendon common to the origin of the supinator and some of the extensor muscles. Specifically, these extensor muscles include the anconeus muscle, the supinator, extensor carpi radialis brevis, extensor digitorum, extensor digiti minimi, and extensor carpi ulnaris. In birds, where the arm is somewhat rotated compared to other tetrapods, it is termed dorsal epicondyle of the humerus. In comparative anatomy, the term ectepicondyle is sometimes used.
The flexor pollicis longus is a muscle in the forearm and hand that flexes the thumb. It lies in the same plane as the flexor digitorum profundus. This muscle is unique to humans, being either rudimentary or absent in other primates. A meta-analysis indicated accessory flexor pollicis longus is present in around 48% of the population.
The pronator teres is a muscle that, along with the pronator quadratus, serves to pronate the forearm. It has two origins, at the medial humeral supracondylar ridge and the ulnar tuberosity, and inserts near the middle of the radius.
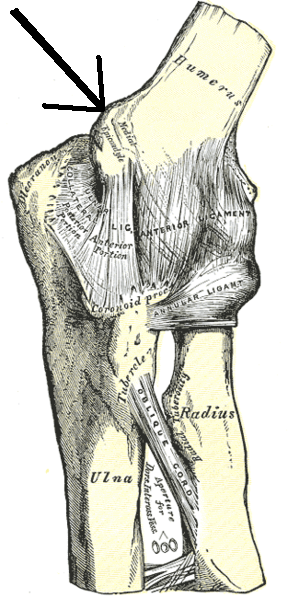
The medial epicondyle of the humerus is an epicondyle of the humerus bone of the upper arm in humans. It is larger and more prominent than the lateral epicondyle and is directed slightly more posteriorly in the anatomical position. In birds, where the arm is somewhat rotated compared to other tetrapods, it is called the ventral epicondyle of the humerus. In comparative anatomy, the more neutral term entepicondyle is used.

The anterior interosseous nerve is a branch of the median nerve that supplies the deep muscles on the anterior of the forearm, except the ulnar (medial) half of the flexor digitorum profundus. Its nerve roots come from C8 and T1.
The posterior compartment of the forearm contains twelve muscles which primarily extend the wrist and digits. It is separated from the anterior compartment by the interosseous membrane between the radius and ulna.

Idiopathic Ulnar neuropathy at the elbow is a condition where pressure on the ulnar nerve as it passes through the cubital tunnel causes nerve dysfunction (neuropathy). The symptoms of neuropathy are paresthesia (tingling) and numbness primarily affecting the little finger and ring finger of the hand. Ulnar neuropathy can progress to weakness and atrophy of the muscles in the hand. Symptoms can be alleviated by attempts to keep the elbow from flexing while sleeping, such as sticking one's arm in the pillow case, so the pillow restricts flexion.
Ulnar neuropathy is a disorder involving the ulnar nerve. Ulnar neuropathy may be caused by entrapment of the ulnar nerve with resultant numbness and tingling. It may also cause weakness or paralysis of the muscles supplied by the nerve.

The elbow is the region between the upper arm and the forearm that surrounds the elbow joint. The elbow includes prominent landmarks such as the olecranon, the cubital fossa, and the lateral and the medial epicondyles of the humerus. The elbow joint is a hinge joint between the arm and the forearm; more specifically between the humerus in the upper arm and the radius and ulna in the forearm which allows the forearm and hand to be moved towards and away from the body. The term elbow is specifically used for humans and other primates, and in other vertebrates it is not used. In those cases, forelimb plus joint is used.
Injuries to the arm, forearm or wrist area can lead to various nerve disorders. One such disorder is median nerve palsy. The median nerve controls the majority of the muscles in the forearm. It controls abduction of the thumb, flexion of hand at wrist, flexion of digital phalanx of the fingers, is the sensory nerve for the first three fingers, etc. Because of this major role of the median nerve, it is also called the eye of the hand. If the median nerve is damaged, the ability to abduct and oppose the thumb may be lost due to paralysis of the thenar muscles. Various other symptoms can occur which may be repaired through surgery and tendon transfers. Tendon transfers have been very successful in restoring motor function and improving functional outcomes in patients with median nerve palsy.

Ulnar collateral ligament injuries can occur during certain activities such as overhead baseball pitching. Acute or chronic disruption of the ulnar collateral ligament result in medial elbow pain, valgus instability, and impaired throwing performance. There are both non-surgical and surgical treatment options.