
Sputum is mucus that is coughed up from the lower airways. In medicine, sputum samples are usually used for a naked eye examination, microbiological investigation of respiratory infections and cytological investigations of respiratory systems. It is crucial that the specimen does not include any mucoid material from the nose or oral cavity.
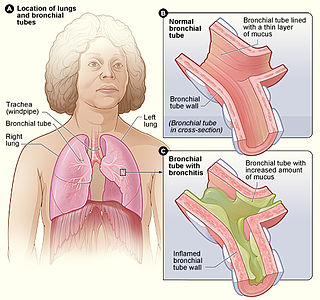
Acute bronchitis, also known as a chest cold, is short-term bronchitis – inflammation of the bronchi of the lungs. The most common symptom is a cough. Other symptoms include coughing up mucus, wheezing, shortness of breath, fever, and chest discomfort. The infection may last from a few to ten days. The cough may persist for several weeks afterward with the total duration of symptoms usually around three weeks. Some have symptoms for up to six weeks.
Salt water aspiration syndrome is a rare diving disorder suffered by scuba divers who inhale a mist of seawater, usually from a faulty demand valve, causing irritation of the lungs. It is not the same thing as aspiration of salt water as a bulk liquid, i.e. drowning. It can usually be treated by rest for several hours. If severe, medical assessment is required. First described by Carl Edmonds.

Granulomatosis with polyangiitis (GPA), also known as Wegener's granulomatosis (WG), after the German physician Friedrich Wegener, is a rare long-term systemic disorder that involves the formation of granulomas and inflammation of blood vessels (vasculitis). It is an autoimmune disease and a form of vasculitis that affects small- and medium-size vessels in many organs but most commonly affects the upper respiratory tract, lungs and kidneys. The signs and symptoms of GPA are highly varied and reflect which organs are supplied by the affected blood vessels. Typical signs and symptoms include nosebleeds, stuffy nose and crustiness of nasal secretions, and inflammation of the uveal layer of the eye. Damage to the heart, lungs and kidneys can be fatal.

A hemothorax is an accumulation of blood within the pleural cavity. The symptoms of a hemothorax may include chest pain and difficulty breathing, while the clinical signs may include reduced breath sounds on the affected side and a rapid heart rate. Hemothoraces are usually caused by an injury, but they may occur spontaneously due to cancer invading the pleural cavity, as a result of a blood clotting disorder, as an unusual manifestation of endometriosis, in response to Pneumothorax, or rarely in association with other conditions.
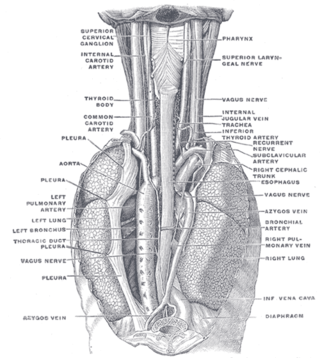
In human anatomy, the bronchial arteries supply the lungs with oxygenated blood, and nutrition. Although there is much variation, there are usually two bronchial arteries that run to the left lung, and one to the right lung, and are a vital part of the respiratory system.

Respiratory diseases, or lung diseases, are pathological conditions affecting the organs and tissues that make gas exchange difficult in air-breathing animals. They include conditions of the respiratory tract including the trachea, bronchi, bronchioles, alveoli, pleurae, pleural cavity, the nerves and muscles of respiration. Respiratory diseases range from mild and self-limiting, such as the common cold, influenza, and pharyngitis to life-threatening diseases such as bacterial pneumonia, pulmonary embolism, tuberculosis, acute asthma, lung cancer, and severe acute respiratory syndromes, such as COVID-19. Respiratory diseases can be classified in many different ways, including by the organ or tissue involved, by the type and pattern of associated signs and symptoms, or by the cause of the disease.

An aspergilloma is a clump of mold which exists in a body cavity such as a paranasal sinus or an organ such as the lung. By definition, it is caused by fungi of the genus Aspergillus.
Rasmussen aneurysm is a distinctive variant of pseudoaneurysm of a branch of the pulmonary artery, predominantly found adjacent to or within a lung cavity, both often arising as a complication of pulmonary tuberculosis. The condition was originally described by Fritz Valdemar Rasmussen in 1868. It is a relatively uncommon complication associated with cavitary tuberculosis of the lung, with its prevalence observed in approximately 5–8% of cases based on autopsy findings.

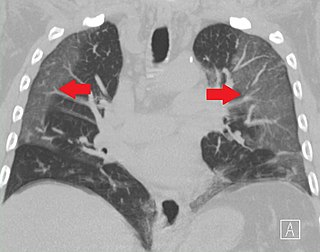
Peribronchial cuffing, also referred to as peribronchial thickening or bronchial wall thickening, is a radiologic sign which occurs when excess fluid or mucus buildup in the small airway passages of the lung causes localized patches of atelectasis. This causes the area around the bronchus to appear more prominent on an X-ray. It has also been described as donut sign, considering the edge is thicker, and the center contains air.
Pulmonary-renal syndrome (PRS) is a rare medical syndrome in which respiratory failure involving bleeding in the lungs and kidney failure (glomerulonephritis) occur. PRS is associated with a high rate of morbidity and death. The term was first used by Goodpasture in 1919 to describe the association of respiratory and kidney failure.

Hughes–Stovin syndrome (HSS) is a rare autoimmune disorder often described as inflammation in relation to blood vessels, a form of vasculitis. It is not associated with any known cause and is typically characterized by multiple aneurysms in pulmonary arteries and deep vein thromboses. It is named after the two British physicians, John Patterson Hughes and Peter George Ingle Stovin, who first described it in 1959. HSS is presumed to be a rare variant of Behçet's disease, which entails more general problems with the circulatory system. Due to its clinical similarity with Behçet's disease, it has also been referred to as 'Incomplete Behçet's disease.' Most patients are young adult males between the age of 20–40. Common clinical presentations include fever, cough, dyspnea and hemoptysis. Radiological features are similar to those of Behçet's disease.

Eosinophilic bronchitis (EB) is a type of airway inflammation due to excessive mast cell recruitment and activation in the superficial airways as opposed to the smooth muscles of the airways as seen in asthma. It often results in a chronic cough. Lung function tests are usually normal. Inhaled corticosteroids are often an effective treatment.
Swimming induced pulmonary edema (SIPE), also known as immersion pulmonary edema, is a life threatening condition that occurs when fluids from the blood leak abnormally from the small vessels of the lung (pulmonary capillaries) into the airspaces (alveoli).

Chronic pulmonary aspergillosis is a long-term fungal infection caused by members of the genus Aspergillus—most commonly Aspergillusfumigatus. The term describes several disease presentations with considerable overlap, ranging from an aspergilloma—a clump of Aspergillus mold in the lungs—through to a subacute, invasive form known as chronic necrotizing pulmonary aspergillosis which affects people whose immune system is weakened. Many people affected by chronic pulmonary aspergillosis have an underlying lung disease, most commonly tuberculosis, allergic bronchopulmonary aspergillosis, asthma, or lung cancer.
Ground-glass opacity (GGO) is a finding seen on chest x-ray (radiograph) or computed tomography (CT) imaging of the lungs. It is typically defined as an area of hazy opacification (x-ray) or increased attenuation (CT) due to air displacement by fluid, airway collapse, fibrosis, or a neoplastic process. When a substance other than air fills an area of the lung it increases that area's density. On both x-ray and CT, this appears more grey or hazy as opposed to the normally dark-appearing lungs. Although it can sometimes be seen in normal lungs, common pathologic causes include infections, interstitial lung disease, and pulmonary edema.
Thoracic endometriosis is a rare form of endometriosis where endometrial-like tissue is found in the lung parenchyma and/or the pleura. It can be classified as either pulmonary, or pleural, respectively. Endometriosis is characterized by the presence of tissue similar to the lining of the uterus forming abnormal growths elsewhere in the body. Usually these growths are found in the pelvis, between the rectum and the uterus, the ligaments of the pelvis, the bladder, the ovaries, and the sigmoid colon. The cause is not known. The most common symptom of thoracic endometriosis is chest pain occurring right before or during menstruation. Diagnosis is based on clinical history and examination, augmented with X-ray, CT scan, and magnetic resonance imaging of the chest. Treatment options include surgery and hormones.
Plastic bronchitis (PB) is a disorder in which branching casts of the airways are expectorated. PB is not a single disease with a defined mechanism that explains the cast formation in all conditions. Examples of diseases associated with expectoration of casts, and which sometimes are labeled PB include tuberculosis, atypical mycobacterial disease, allergic bronchopulmonary aspergillosis, and asthma.

A lung cavity or pulmonary cavity is an abnormal, thick-walled, air-filled space within the lung. Cavities in the lung can be caused by infections, cancer, autoimmune conditions, trauma, congenital defects, or pulmonary embolism. The most common cause of a single lung cavity is lung cancer. Bacterial, mycobacterial, and fungal infections are common causes of lung cavities. Globally, tuberculosis is likely the most common infectious cause of lung cavities. Less commonly, parasitic infections can cause cavities. Viral infections almost never cause cavities. The terms cavity and cyst are frequently used interchangeably; however, a cavity is thick walled, while a cyst is thin walled. The distinction is important because cystic lesions are unlikely to be cancer, while cavitary lesions are often caused by cancer.
Bronchial artery embolization is a treatment for hemoptysis, abbreviated as BAE. It is a kind of catheter intervention to control hemoptysis by embolizing the bronchial artery, which is a bleeding source. Embolic agents are particulate embolic material such as gelatin sponge or polyvinyl alcohol (PVA), and liquid embolic material such as NBCA, or metallic coils.


