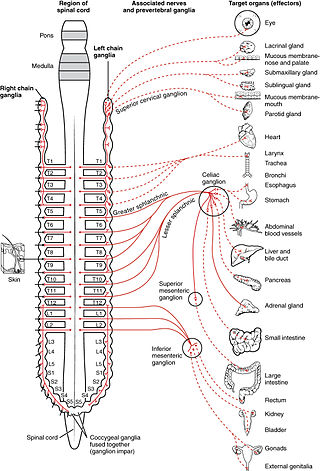
The sympathetic nervous system (SNS) is one of the three divisions of the autonomic nervous system, the others being the parasympathetic nervous system and the enteric nervous system. The enteric nervous system is sometimes considered part of the autonomic nervous system, and sometimes considered an independent system.

Mydriasis is the dilation of the pupil, usually having a non-physiological cause, or sometimes a physiological pupillary response. Non-physiological causes of mydriasis include disease, trauma, or the use of certain types of drug. It may also be of unknown cause.

The pupillary light reflex (PLR) or photopupillary reflex is a reflex that controls the diameter of the pupil, in response to the intensity (luminance) of light that falls on the retinal ganglion cells of the retina in the back of the eye, thereby assisting in adaptation of vision to various levels of lightness/darkness. A greater intensity of light causes the pupil to constrict, whereas a lower intensity of light causes the pupil to dilate. Thus, the pupillary light reflex regulates the intensity of light entering the eye. Light shone into one eye will cause both pupils to constrict.

Miosis, or myosis, is excessive constriction of the pupil. The opposite condition, mydriasis, is the dilation of the pupil. Anisocoria is the condition of one pupil being more dilated than the other.

A Pancoast tumor is a tumor of the apex of the lung. It is a type of lung cancer defined primarily by its location situated at the top end of either the right or left lung. It typically spreads to nearby tissues such as the ribs and vertebrae. Most Pancoast tumors are non-small-cell lung cancers.
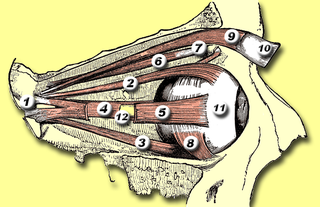
The levator palpebrae superioris is the muscle in the orbit that elevates the upper eyelid.

Harlequin syndrome is a condition characterized by asymmetric sweating and flushing on the upper thoracic region of the chest, neck and face. Harlequin syndrome is considered an injury to the autonomic nervous system (ANS). The ANS controls some of the body's natural processes such as sweating, skin flushing and pupil response to stimuli. Individuals with this syndrome have an absence of sweat skin flushing unilaterally, usually on one side of the face, arms and chest. It is an autonomic disorder that may occur at any age. Harlequin syndrome affects fewer than 1000 people in the United States.

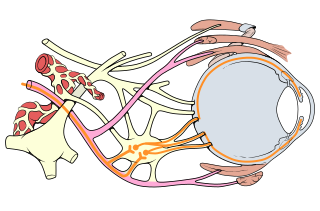
The ciliary ganglion is a bundle of nerves, parasympathetic ganglion located just behind the eye in the posterior orbit. It is 1–2 mm in diameter and in humans contains approximately 2,500 neurons. The ganglion contains postganglionic parasympathetic neurons. These neurons supply the pupillary sphincter muscle, which constricts the pupil, and the ciliary muscle which contracts to make the lens more convex. Both of these muscles are involuntary since they are controlled by the parasympathetic division of the autonomic nervous system.

Adie syndrome, also known as Holmes–Adie syndrome, is a neurological disorder characterized by a tonically dilated pupil that reacts slowly to light but shows a more definite response to accommodation. It is frequently seen in females with absent knee or ankle jerks and impaired sweating.

Anisocoria is a condition characterized by an unequal size of the eyes' pupils. Affecting up to 20% of the population, anisocoria is often entirely harmless, but can be a sign of more serious medical problems.
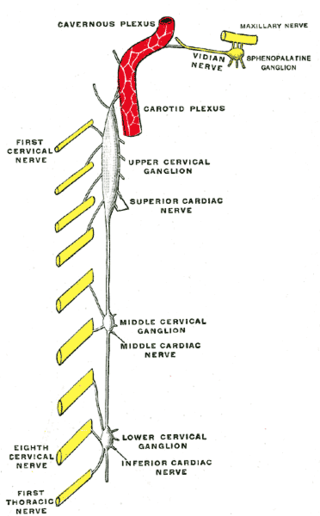
The superior cervical ganglion (SCG) is the upper-most and largest of the cervical sympathetic ganglia of the sympathetic trunk. It probably formed by the union of four sympathetic ganglia of the cervical spinal nerves C1–C4. It is the only ganglion of the sympathetic nervous system that innervates the head and neck. The SCG innervates numerous structures of the head and neck.
The orbitalis muscle is a vestigial or rudimentary nonstriated muscle that crosses from the infraorbital groove and sphenomaxillary fissure and is intimately united with the periosteum of the orbit. It was described by Heinrich Müller and is often called Müller's muscle. It lies at the back of the orbit and spans the infraorbital fissure. It is a thin layer of smooth muscle that bridges the inferior orbital fissure. It is supplied by sympathetic nerves, and its function is unknown.

Ptosis, also known as blepharoptosis, is a drooping or falling of the upper eyelid. This condition is sometimes called "lazy eye," but that term normally refers to the condition amblyopia. If severe enough and left untreated, the drooping eyelid can cause other conditions, such as amblyopia or astigmatism, so it is especially important to treat the disorder in children before it can interfere with vision development.
Hypohidrosis is a disorder in which a person exhibits diminished sweating in response to appropriate stimuli. In contrast with hyperhidrosis, which is a socially troubling yet often benign condition, the consequences of untreated hypohidrosis include hyperthermia, heat stroke and death. An extreme case of hypohidrosis in which there is a complete absence of sweating and the skin is dry is termed anhidrosis.
Oculomotor nerve palsy or oculomotor neuropathy is an eye condition resulting from damage to the third cranial nerve or a branch thereof. As the name suggests, the oculomotor nerve supplies the majority of the muscles controlling eye movements. Damage to this nerve will result in an inability to move the eye normally. The nerve also supplies the upper eyelid muscle and is accompanied by parasympathetic fibers innervating the muscles responsible for pupil constriction. The limitations of eye movement resulting from the condition are generally so severe that patients are often unable to maintain normal eye alignment when gazing straight ahead, leading to strabismus and, as a consequence, double vision (diplopia).

The lumbar ganglia are paravertebral ganglia located in the inferior portion of the sympathetic trunk. The lumbar portion of the sympathetic trunk typically has 4 lumbar ganglia. The lumbar splanchnic nerves arise from the ganglia here, and contribute sympathetic efferent fibers to the nearby plexuses. The first two lumbar ganglia have both white and gray rami communicates.
Babinski–Nageotte syndrome is an alternating brainstem syndrome. It occurs when there is damage to the dorsolateral or posterior lateral medulla oblongata, likely syphilitic in origin. Hence it is also called the alternating medulla oblongata syndrome.
The hypothalamospinal tract is a nerve tract that arises mainly from the paraventricular nucleus of hypothalamus, and lateral and posterior areas of the hypothalamus. The tract descends through the periaqueductal gray and adjacent reticular formation. It is found in the dorsolateral quadrant of the lateral funiculus, in the lateral tegmentum of the medulla, pons and midbrain.
Villaret's syndrome combines ipsilateral paralysis of the last four cranial nerves and Horner syndrome. Sometimes cranial nerve VII is also involved. It may also involve the cervical ganglia of the sympathetic trunk. Paralysis is caused by a lesion in the retroparotid space, which is bounded posteriorly by the cervical vertebrae, superiorly by the skull near the jugular foramen, anteriorly by the parotid gland, laterally by the sternocleidomastoid muscle, and medially by the pharynx.

The ciliary ganglion is a parasympathetic ganglion located just behind the eye in the posterior orbit. Three types of axons enter the ciliary ganglion but only the preganglionic parasympathetic axons synapse there. The entering axons are arranged into three roots of the ciliary ganglion, which join enter the posterior surface of the ganglion.


