
The pupil is a black hole located in the center of the iris of the eye that allows light to strike the retina. It appears black because light rays entering the pupil are either absorbed by the tissues inside the eye directly, or absorbed after diffuse reflections within the eye that mostly miss exiting the narrow pupil. The size of the pupil is controlled by the iris, and varies depending on many factors, the most significant being the amount of light in the environment. The term "pupil" was coined by Gerard of Cremona.
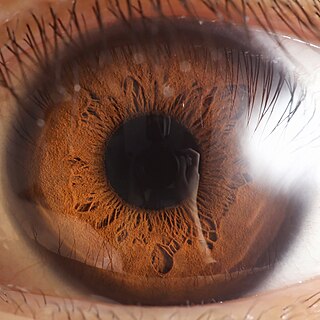
In humans and most mammals and birds, the iris is a thin, annular structure in the eye, responsible for controlling the diameter and size of the pupil, and thus the amount of light reaching the retina. Eye color is defined by the iris. In optical terms, the pupil is the eye's aperture, while the iris is the diaphragm.
Mydriasis is the dilation of the pupil, usually having a non-physiological cause, or sometimes a physiological pupillary response. Non-physiological causes of mydriasis include disease, trauma, or the use of certain types of drug. It may also be of unknown cause.
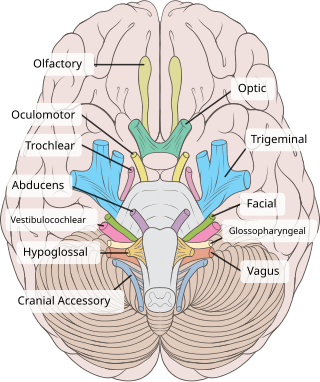
The oculomotor nerve, also known as the third cranial nerve, cranial nerve III, or simply CN III, is a cranial nerve that enters the orbit through the superior orbital fissure and innervates extraocular muscles that enable most movements of the eye and that raise the eyelid. The nerve also contains fibers that innervate the intrinsic eye muscles that enable pupillary constriction and accommodation. The oculomotor nerve is derived from the basal plate of the embryonic midbrain. Cranial nerves IV and VI also participate in control of eye movement.
Cycloplegia is paralysis of the ciliary muscle of the eye, resulting in a loss of accommodation. Because of the paralysis of the ciliary muscle, the curvature of the lens can no longer be adjusted to focus on nearby objects. This results in similar problems as those caused by presbyopia, in which the lens has lost elasticity and can also no longer focus on close-by objects. Cycloplegia with accompanying mydriasis is usually due to topical application of muscarinic antagonists such as atropine and cyclopentolate.

The pupillary light reflex (PLR) or photopupillary reflex is a reflex that controls the diameter of the pupil, in response to the intensity (luminance) of light that falls on the retinal ganglion cells of the retina in the back of the eye, thereby assisting in adaptation of vision to various levels of lightness/darkness. A greater intensity of light causes the pupil to constrict, whereas a lower intensity of light causes the pupil to dilate. Thus, the pupillary light reflex regulates the intensity of light entering the eye. Light shone into one eye will cause both pupils to constrict.

Argyll Robertson pupils are bilateral small pupils that reduce in size on a near object, but do not constrict when exposed to bright light. They are a highly specific sign of neurosyphilis; however, Argyll Robertson pupils may also be a sign of diabetic neuropathy. In general, pupils that accommodate but do not react are said to show light-near dissociation (i.e., it is the absence of a miotic reaction to light, both direct and consensual, with the preservation of a miotic reaction to near stimulus.

Miosis, or myosis, is excessive constriction of the pupil. The opposite condition, mydriasis, is the dilation of the pupil. Anisocoria is the condition of one pupil being more dilated than the other.

Horner's syndrome, also known as oculosympathetic paresis, is a combination of symptoms that arises when a group of nerves known as the sympathetic trunk is damaged. The signs and symptoms occur on the same side (ipsilateral) as it is a lesion of the sympathetic trunk. It is characterized by miosis, partial ptosis, apparent anhidrosis, with apparent enophthalmos.

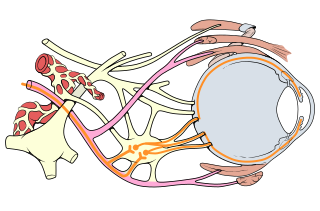
The ciliary ganglion is a bundle of nerves, parasympathetic ganglion located just behind the eye in the posterior orbit. It is 1–2 mm in diameter and in humans contains approximately 2,500 neurons. The ganglion contains postganglionic parasympathetic neurons. These neurons supply the pupillary sphincter muscle, which constricts the pupil, and the ciliary muscle which contracts to make the lens more convex. Both of these muscles are involuntary since they are controlled by the parasympathetic division of the autonomic nervous system.

Adie syndrome, also known as Holmes-Adie syndrome, is a neurological disorder characterized by a tonically dilated pupil that reacts slowly to light but shows a more definite response to accommodation. It is frequently seen in females with absent knee or ankle jerks and impaired sweating.

Parinaud's syndrome is a constellation of neurological signs indicating injury to the dorsal midbrain. More specifically, compression of the vertical gaze center at the rostral interstitial nucleus of medial longitudinal fasciculus (riMLF).

A relative afferent pupillary defect (RAPD), also known as a Marcus Gunn pupil, is a medical sign observed during the swinging-flashlight test whereupon the patient's pupils dilate when a bright light is swung from the unaffected eye to the affected eye. The affected eye still senses the light and produces pupillary sphincter constriction to some degree, albeit reduced.
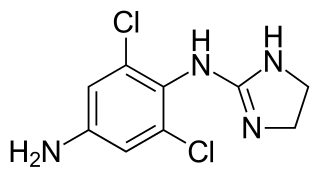
Apraclonidine (INN), also known under the brand name Iopidine, is a sympathomimetic used in glaucoma therapy. It is an α2 adrenergic receptor agonist and a weak α1 adrenergic receptor agonist.

Ptosis, also known as blepharoptosis, is a drooping or falling of the upper eyelid. This condition is sometimes called "lazy eye," but that term normally refers to the condition amblyopia. If severe enough and left untreated, the drooping eyelid can cause other conditions, such as amblyopia or astigmatism, so it is especially important to treat the disorder in children before it can interfere with vision development.

Weber's syndrome, also known as midbrain stroke syndrome or superior alternating hemiplegia, is a form of stroke that affects the medial portion of the midbrain. It involves oculomotor fascicles in the interpeduncular cisterns and cerebral peduncle so it characterizes the presence of an ipsilateral lower motor neuron type oculomotor nerve palsy and contralateral hemiparesis or hemiplegia.
Oculomotor nerve palsy or oculomotor neuropathy is an eye condition resulting from damage to the third cranial nerve or a branch thereof. As the name suggests, the oculomotor nerve supplies the majority of the muscles controlling eye movements. Damage to this nerve will result in an inability to move the eye normally. The nerve also supplies the upper eyelid muscle and is accompanied by parasympathetic fibers innervating the muscles responsible for pupil constriction. The limitations of eye movement resulting from the condition are generally so severe that patients are often unable to maintain normal eye alignment when gazing straight ahead, leading to strabismus and, as a consequence, double vision (diplopia).

Pupillary response is a physiological response that varies the size of the pupil, via the optic and oculomotor cranial nerve.
The eye is made up of the sclera, the iris, and the pupil, a black hole located at the center of the eye with the main function of allowing light to pass to the retina. Due to certain muscle spasms in the eye, the pupil can resemble a tadpole, which consists of a circular body, no arms or legs, and a tail.
Physiological anisocoria is when human pupils differ in size. It is generally considered to be benign, though it must be distinguished from Congenital Horner's syndrome, pharmacological dilatation or other conditions connected to the sympathetic nervous system. The prevalence of physiological anisocoria has not been found to be influenced by the sex, age, or iris color of the subject.
