
Conjunctivitis, also known as pink eye, is inflammation of the outermost layer of the white part of the eye and the inner surface of the eyelid. It makes the eye appear pink or reddish. Pain, burning, scratchiness, or itchiness may occur. The affected eye may have increased tears or be "stuck shut" in the morning. Swelling of the white part of the eye may also occur. Itching is more common in cases due to allergies. Conjunctivitis can affect one or both eyes.
An allergen is a type of antigen that produces an abnormally vigorous immune response in which the immune system fights off a perceived threat that would otherwise be harmless to the body. Such reactions are called allergies.

Mastocytosis, a type of mast cell disease, is a rare disorder affecting both children and adults caused by the accumulation of functionally defective mast cells and CD34+ mast cell precursors.
H1 antagonists, also called H1 blockers, are a class of medications that block the action of histamine at the H1 receptor, helping to relieve allergic reactions. Agents where the main therapeutic effect is mediated by negative modulation of histamine receptors are termed antihistamines; other agents may have antihistaminergic action but are not true antihistamines.

Allergic rhinitis, of which the seasonal type is called hay fever, is a type of inflammation in the nose that occurs when the immune system overreacts to allergens in the air. Signs and symptoms include a runny or stuffy nose, sneezing, red, itchy, and watery eyes, and swelling around the eyes. The fluid from the nose is usually clear. Symptom onset is often within minutes following allergen exposure, and can affect sleep and the ability to work or study. Some people may develop symptoms only during specific times of the year, often as a result of pollen exposure. Many people with allergic rhinitis also have asthma, allergic conjunctivitis, or atopic dermatitis.

Rhinitis, also known as coryza, is irritation and inflammation of the mucous membrane inside the nose. Common symptoms are a stuffy nose, runny nose, sneezing, and post-nasal drip.

Hives, also known as urticaria, is a kind of skin rash with red, raised, itchy bumps. Hives may burn or sting. The patches of rash may appear on different body parts, with variable duration from minutes to days, and does not leave any long-lasting skin change. Fewer than 5% of cases last for more than six weeks. The condition frequently recurs.
Type I hypersensitivity, in the Gell and Coombs classification of allergic reactions, is an allergic reaction provoked by re-exposure to a specific type of antigen referred to as an allergen. Type I is distinct from type II, type III and type IV hypersensitivities. The relevance of the Gell and Coombs classification of allergic reactions has been questioned in the modern-day understanding of allergy, and it has limited utility in clinical practice.
Keratoconjunctivitis is inflammation ("-itis") of the cornea and conjunctiva.
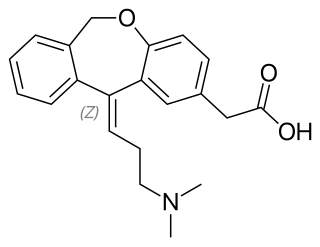
Olopatadine, sold under the brand name Opatanol among others, is a medication used to decrease the symptoms of allergic conjunctivitis and allergic rhinitis. It is used as eye drops or as a nasal spray. The eye drops generally result in an improvement within half an hour.

Ketotifen, sold under the brand name Zaditor among others, is a second-generation noncompetitive H1-antihistamine and mast cell stabilizer. It is most commonly sold as a salt with fumaric acid, ketotifen fumarate, and is available in two forms. In its ophthalmic form, it is used to treat allergic conjunctivitis. In its oral form, it is used to prevent asthma attacks or anaphylaxis, as well as various mast cell, allergic-type disorders.

Vernal keratoconjunctivitis is a recurrent, bilateral, and self-limiting type of conjunctivitis having a periodic seasonal incidence.

Emedastine (trade name Emadine) is a second generation antihistamine used in eye drops to alleviate the symptoms of allergic conjunctivitis. It acts as a H1 receptor antagonist. It works by blocking the action of histamine that causes allergic symptoms. It is used in form of the difumarate. The emedastine difumarate is a white, crystalline, water-soluble fine powder. Emedastine eye drops is usually applied twice a day to the affected eye. When the patients with allergic conjunctivitis were treated with 0.05% emedastine difumarate ophthalmic solution for six weeks, the signs and symptoms such as redness, itching and swelling of the eyes were relieved. Emedastine appears to be devoid of effects on adrenergic, dopaminergic and serotonin receptors. This drug was developed by Alcon, which is global medical company specializing in eye care products.

Allergic inflammation is an important pathophysiological feature of several disabilities or medical conditions including allergic asthma, atopic dermatitis, allergic rhinitis and several ocular allergic diseases. Allergic reactions may generally be divided into two components; the early phase reaction, and the late phase reaction. While the contribution to the development of symptoms from each of the phases varies greatly between diseases, both are usually present and provide us a framework for understanding allergic disease.

Mast cell stabilizers are medications used to prevent or control certain allergic disorders. They block mast cell degranulation, stabilizing the cell and thereby preventing the release of histamine and related mediators. One suspected pharmacodynamic mechanism is the blocking of IgE-regulated calcium channels. Without intracellular calcium, the histamine vesicles cannot fuse to the cell membrane and degranulate.
A drug allergy is an allergy to a drug, most commonly a medication, and is a form of adverse drug reaction. Medical attention should be sought immediately if an allergic reaction is suspected.

Antihistamines are drugs which treat allergic rhinitis, common cold, influenza, and other allergies. Typically, people take antihistamines as an inexpensive, generic drug that can be bought without a prescription and provides relief from nasal congestion, sneezing, or hives caused by pollen, dust mites, or animal allergy with few side effects. Antihistamines are usually for short-term treatment. Chronic allergies increase the risk of health problems which antihistamines might not treat, including asthma, sinusitis, and lower respiratory tract infection. Consultation of a medical professional is recommended for those who intend to take antihistamines for longer-term use.

An allergic response is a hypersensitive immune reaction to a substance that normally is harmless or would not cause an immune response in everyone. An allergic response may cause harmful symptoms such as itching or inflammation or tissue injury.

Alcaftadine is used to prevent eye irritation brought on by allergic conjunctivitis. It is a H1 histamine receptor antagonist.
Mast cell activation syndrome (MCAS) is a term referring to one of two types of mast cell activation disorder (MCAD); the other type is idiopathic MCAD. MCAS is an immunological condition in which mast cells inappropriately and excessively release chemical mediators, resulting in a range of chronic symptoms, sometimes including anaphylaxis or near-anaphylaxis attacks. Primary symptoms include cardiovascular, dermatological, gastrointestinal, neurological and respiratory problems.

