
Allergies, also known as allergic diseases, are various conditions caused by hypersensitivity of the immune system to typically harmless substances in the environment. These diseases include hay fever, food allergies, atopic dermatitis, allergic asthma, and anaphylaxis. Symptoms may include red eyes, an itchy rash, sneezing, coughing, a runny nose, shortness of breath, or swelling. Note that food intolerances and food poisoning are separate conditions.
An allergen is a type of antigen that produces an abnormally vigorous immune response in which the immune system fights off a perceived threat that would otherwise be harmless to the body. Such reactions are called allergies.
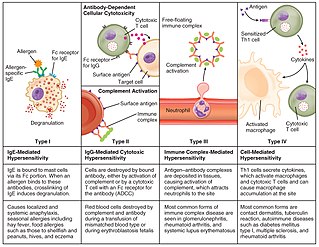
Hypersensitivity is an abnormal physiological condition in which there is an undesirable and adverse immune response to antigen. It is an abnormality in the immune system that causes immune diseases including allergies and autoimmunity. It is caused by many types of particles and substances from the external environment or from within the body that are recognized by the immune cells as antigens. The immune reactions are usually referred to as an over-reaction of the immune system and they are often damaging and uncomfortable.

A food allergy is an abnormal immune response to food. The symptoms of the allergic reaction may range from mild to severe. They may include itchiness, swelling of the tongue, vomiting, diarrhea, hives, trouble breathing, or low blood pressure. This typically occurs within minutes to several hours of exposure. When the symptoms are severe, it is known as anaphylaxis. A food intolerance and food poisoning are separate conditions, not due to an immune response.

Contact dermatitis is a type of acute or chronic inflammation of the skin caused by exposure to chemical or physical agents. Symptoms of contact dermatitis can include itchy or dry skin, a red rash, bumps, blisters, or swelling. These rashes are not contagious or life-threatening, but can be very uncomfortable.

Atopy is the tendency to produce an exaggerated immunoglobulin E (IgE) immune response to otherwise harmless substances in the environment. Allergic diseases are clinical manifestations of such inappropriate, atopic responses.

A hypoallergenic dog breed is a dog breed that is purportedly more compatible with allergic people than are other breeds. However, prominent allergen researchers have determined that there is no basis to the claims that certain breeds are hypoallergenic and, while allergen levels vary among individual dogs, the breed is not a significant factor.

A patch test is a diagnostic method used to determine which specific substances cause allergic inflammation of a patient's skin.

Peanut allergy is a type of food allergy to peanuts. It is different from tree nut allergies, because peanuts are legumes and not true nuts. Physical symptoms of allergic reaction can include itchiness, hives, swelling, eczema, sneezing, asthma attack, abdominal pain, drop in blood pressure, diarrhea, and cardiac arrest. Anaphylaxis may occur. Those with a history of asthma are more likely to be severely affected.

Allergic contact dermatitis (ACD) is a form of contact dermatitis that is the manifestation of an allergic response caused by contact with a substance; the other type being irritant contact dermatitis (ICD).

Milk allergy is an adverse immune reaction to one or more proteins in cow's milk. Symptoms may take hours to days to manifest, with symptoms including atopic dermatitis, inflammation of the esophagus, enteropathy involving the small intestine and proctocolitis involving the rectum and colon. However, rapid anaphylaxis is possible, a potentially life-threatening condition that requires treatment with epinephrine, among other measures.

Wheat allergy is an allergy to wheat which typically presents itself as a food allergy, but can also be a contact allergy resulting from occupational exposure. Like all allergies, wheat allergy involves immunoglobulin E and mast cell response. Typically the allergy is limited to the seed storage proteins of wheat. Some reactions are restricted to wheat proteins, while others can react across many varieties of seeds and other plant tissues. Wheat allergy is rare. Prevalence in adults was found to be 0.21% in a 2012 study in Japan.

Pro-hevein is a wound-induced and a lectin-like protein from Hevea brasiliensis where it is involved in the coagulation of latex.

Ara h 1 is a seed storage protein from Arachis hypogaea (peanuts). It is a heat stable 7S vicilin-like globulin with a stable trimeric form that comprises 12-16% of the total protein in peanut extracts. Ara h 1 is known because sensitization to it was found in 95% of peanut-allergic patients from North America. In spite of this high percentage, peanut-allergic patients of European populations have fewer sensitizations to Ara h 1.
Nickel allergy is any of several allergic conditions provoked by exposure to the chemical element nickel. Nickel allergy often takes the form of nickel allergic contact dermatitis (Ni-ACD), a form of allergic contact dermatitis (ACD). Ni-ACD typically causes a rash that is red and itchy and that may be bumpy or scaly. The main treatment for it is avoiding contact with nickel-releasing metals, such as inexpensive jewelry. Another form of nickel allergy is a systemic form: systemic nickel allergy syndrome (SNAS) can mimic some of the symptoms of irritable bowel syndrome (IBS) and also has a dermatologic component.

Fish allergy is an immune hypersensitivity to proteins found in fish. Symptoms can be either rapid or gradual in onset. The latter can take hours to days to appear. The former may include anaphylaxis, a potentially life-threatening condition which requires treatment with epinephrine. Other presentations may include atopic dermatitis or inflammation of the esophagus. Fish is one of the eight common food allergens which are responsible for 90% of allergic reactions to foods: cow's milk, eggs, wheat, shellfish, peanuts, tree nuts, fish, and soy beans.

Dust mite allergy, also known as house dust allergy, is a sensitization and allergic reaction to the droppings of house dust mites. The allergy is common and can trigger allergic reactions such as asthma, eczema or itching. The mite's gut contains potent digestive enzymes that persist in their feces and are major inducers of allergic reactions such as wheezing. The mite's exoskeleton can also contribute to allergic reactions. Unlike scabies mites or skin follicle mites, house dust mites do not burrow under the skin and are not parasitic.

Shellfish allergy is among the most common food allergies. "Shellfish" is a colloquial and fisheries term for aquatic invertebrates used as food, including various species of molluscs such as clams, mussels, oysters and scallops, crustaceans such as shrimp, lobsters and crabs, and cephalopods such as squid and octopus. Shellfish allergy is an immune hypersensitivity to proteins found in shellfish. Symptoms can be either rapid or gradual in onset. The latter can take hours to days to appear. The former may include anaphylaxis, a potentially life-threatening condition which requires treatment with epinephrine. Other presentations may include atopic dermatitis or inflammation of the esophagus. Shellfish is one of the eight common food allergens, responsible for 90% of allergic reactions to foods: cow's milk, eggs, wheat, shellfish, peanuts, tree nuts, fish, and soy beans.
Metal allergies inflame the skin after it has been in contact with metal. They are a form of allergic contact dermatitis. They are becoming more common, as of 2021, except in areas with regulatory countermeasures.

