The main types of kidney cancer are renal cell cancer (RCC), transitional cell cancer (TCC), and Wilms' tumor.[7] RCC makes up approximately 80% of kidney cancers, and TCC accounts for most of the rest.[8] Risk factors for RCC and TCC include smoking, certain pain medications, previous bladder cancer, being overweight, high blood pressure, certain chemicals, and a family history.[1][2] Risk factors for Wilms' tumor include a family history and certain genetic disorders such as WAGR syndrome.[3] Diagnosis may be suspected based on symptoms, urine testing, and medical imaging.[1][2][3] It is confirmed by tissue biopsy.[1][2][3]
Treatment may include surgery, radiation therapy, chemotherapy, immunotherapy, and targeted therapy.[1][2][3] Kidney cancer newly affected about 403,300 people and resulted in 175,000 deaths globally in 2018.[5] Onset is usually after the age of 45.[4] Males are affected more often than females.[4] The overall five-year survival rate is 75% in the United States, 71% in Canada, 70% in China, and 60% in Europe.[4][9][10][11] For cancers that are confined to the kidney, the five-year survival rate is 93%, if it has spread to the surrounding lymph nodes it is 70%, and if it has spread widely, it is 12%.[4] Kidney cancer has been identified as the 13th most common form of cancer,[12] and is responsible for 2% of the world's cancer cases and deaths.[13] The incidence of kidney cancer has continued to increase since 1930. Renal cancer is more commonly found in populations of urban areas than rural areas.[14]
Signs and symptoms
Early on, kidney masses do not typically cause any symptoms and are undetectable on physical examination.[15] As kidney cancer becomes more advanced it classically results in blood in the urine, flank or back pain, and a mass.[15] Other symptoms that are consistent with advanced disease include weight loss, fever, night sweats, palpable swollen lymph nodes in the neck, non-reducing varicocele, bone pain, continuous cough, and bilateral lower leg swelling.[15][16][17]
The classic triad of visible blood in the urine (hematuria), flank pain and palpable abdominal mass occurs in less than 15% of the cases. RCC may present with signs and symptoms caused by the substances the cancer cell produce (i.e. paraneoplastic syndromes).[citation needed]
Paraneoplastic syndromes caused by kidney cancer can be broadly classified as endocrine and non-endocrine. Endocrine dysfunctions include increase in blood calcium levels (hypercalcemia), high blood pressure (hypertension), increased red bloods (polycythemia), liver dysfunction, milky nipple discharge unrelated normal breast-feeding (galactorrhea), and Cushing's syndrome. Non-endocrine dysfunctions include deposition of protein in tissue (amyloidosis), decrease in hemoglobin or red blood cells (anemia), disorders of nerves, muscles (neuromyopathies), blood vessels (vasculopathy) and blood clotting mechanisms (coagulopathy).[18]
Causes
Factors that increase the risk of kidney cancer include smoking, high blood pressure, obesity, faulty genes, a family history of kidney cancer, having kidney disease that needs dialysis, being infected with hepatitis C, and previous treatment for testicular cancer or cervical cancer.[19][20]
There are also other possible risk factors such as kidney stones being investigated.[21][22]
About 25-30% of kidney cancer is attributed to smoking.[20] Smokers have a 1.3 times higher risk of developing kidney cancer compared to non-smokers. Moreover, there is a dose-dependent increased risk of cancer development. Men who smoke more than 20 cigarettes per day have twice the risk. Likewise, women who smoke more than 20 cigarettes per day have 1.5 times the risk of non-smokers. After 10 years of smoking cessation a substantial reduction is seen in the risk of developing kidney cancer.[23]
Diagnosis
Due to the increase in ultrasound and CT imaging for nonspecific abdominal complaints, kidney masses are frequently incidentally diagnosed on medical imaging.[15][24][25] More than 60% of renal cell carcinoma (the most common type of kidney cancer), are diagnosed incidentally by abdominal imaging for nonspecific abdominal complaints.[15][26]
Kidney masses can be classified by the nature of the cells in the growth, or by its appearance on radiography.[15] The term cancer refers to a malignant tumor, which is an uncontrolled growth of abnormal cells.[27] However, kidney masses can be due to growth of normal tissue (benign), inflammatory (a reaction of the immune system), or vascular (cells of the blood vessels).[citation needed]
Medical imaging
Since there is a large differential diagnosis for a kidney tumor, the first step is to characterize the mass with medical imaging to assess its likelihood of being benign or malignant. Ultrasonography is sometimes used to evaluate a suspected kidney mass, as it can characterize cystic and solid kidney masses without radiation exposure and at relative low cost.[15] Radiologically tumors are grouped based on appearance into simple cystic, complex cystic, or solid.[15] The most important differentiating feature of a cancerous and non-cancerous tumor on imaging is enhancement.[28] Simple cysts, which are defined by strict criteria[29] are safe to be monitored if the person does not have any symptoms.[15] However, all masses that are not clearly simple cysts should be further evaluated and confirmed by alternate imaging techniques.[30][15]
Computed tomography (CT) of the abdomen administered with and without IV contrast is the ideal imaging to diagnose and stage kidney cancer.[31][30][15] There is tentative evidence that iodinated contrast agents may cause worsening of kidney function in people with chronic kidney disease (CKD) with a glomerular filtration rate (GFR) less than 45ml/min/1.73m2 and should therefore be given cautiously in this group.[32]
Abdominal magnetic resonance imaging (MRI) is an alternative imaging method that can be used to characterize and stage a kidney mass.[31][30][15] It may be suggested if contrast material cannot be given.[31] MRI can also evaluate the inferior vena cava if the mass is suspected to extend outside the kidney.[31]
Since the lungs are the most common organ for kidney cancer to spread to, a chest X-ray or CT scan may be ordered based on the person's risk for metastatic disease.[15][30]
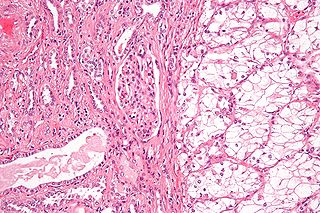
The most common type of kidney malignancy is renal cell carcinoma,[33] which is thought to originate from cells in the proximal convoluted tubule of the nephron.[15][34] Another type of kidney cancer although less common, is transitional cell cancer (TCC) or urothelial carcinoma of the renal pelvis.[35] The renal pelvis is the part of the kidney that collects urine and drains it into a tube called the ureter.[35] The cells that line the renal pelvis are called transitional cells, and are also sometimes called urothelial cells. The transitional/urothelial cells in the renal pelvis are the same type of cells that line the ureter and bladder. For this reason TCC of the renal pelvis is distinct from RCC and is thought to behave more like bladder cancer.[35] Other rare types of kidney cancers that can arise from the urothelial cells of the renal pelvis are squamous cell carcinoma and adenocarcinoma.[15]
Other causes of kidney cancer include the following:[15]
Sarcoma- for example leiomyosarcoma, liposarcoma, angiosarcoma, clear-cell sarcoma and rhabdomyosarcoma are types of sarcomas that have occurred in the kidney
Inverted urothelial papilloma- was traditionally regarded as a benign growth. However, there may be an increased risk for recurrence and transformation to TCC.[38]
In children, Wilms tumor is the most common type of kidney cancer.[15]Mesoblastic nephroma, although rare, also typically presents in childhood.
Renal cell carcinoma has been further divided into sub-types based on histological features and genetic abnormalities. The 2004 WHO Classification of the Renal Tumors of the Adults describes these categories:[39]
People with suspected kidney cancer should also have their kidney function evaluated to help determine treatment options. Blood tests to determine kidney function include a comprehensive metabolic panel (CMP), a complete blood count (CBC).[43][30] In addition, these tests help understand the overall health of the person, which can be affected by metastatic disease (disease that is outside of the kidney). For example, liver or bone involvement could result in abnormal liver enzymes, electrolyte abnormalities, or anemia. A urine sample should also be collected for urinalysis.[30][15]
Biopsy
The utility of renal mass biopsy (RMB) lies in that it can confirm malignancy with reliability, can direct therapy based on diagnosis, and can provide drainage.[30]
Once imaging has been completed, renal mass biopsy should be considered if there is a high likelihood that the mass is hematologic, metastatic, inflammatory, or infectious.[30] These types of lesions would not be managed surgically, differing from cancer originating from the kidney. Cancer originating outside the kidney and lymphoma are managed systemically.[15][30]
RMB can accurately diagnose malignancy, however, it cannot reliably diagnose benign disease. In other words, if the biopsy shows cancer, there is a 99.8% chance that kidney cancer is present (Positive Predictive Value= 99.8%). A negative biopsy does not rule out a diagnosis of cancer.[44]
Staging
Staging is the process that helps determine the extent and spread of the disease.[45] Renal cell carcinoma is the only type of kidney cancer that can be staged. The first step of staging follows the TNM staging system proposed by the Union International Contre le Cancer that is widely used among cancers in other organs.[15] The TNM staging system classifies the primary tumor (T), lymph nodes (N) and distant metastasis (M) of the disease. The American Joint Committee on Cancer (AJCC) published a Cancer Staging Manual revision in 2010 that describes the values of TMN for renal cell carcinoma.[46][15]
Lymph node involvement is classified as either regional lymph node metastasis (N1), or no involvement (N0).[46] Similarly, M1 describes distant metastasis, while M0 describes no distant metastasis.[46]
The primary tumor of renal cell carcinoma is categorized in the table below, as according to the AJCC 8th Edition Cancer Staging Manual:[47][48]
Stage
TNM
Description
Tx, N0, M0
Tumor cannot be assessed
T0, N0, M0
No evidence of primary tumor
I
T1, N0, M0
Tumor ≤7cm; limited to kidney
T1a, N0, M0
Tumor ≤4cm; limited to kidney
T1b, N0, M0
Tumor 4-≤7cm; limited to kidney
II
T2, N0, M0
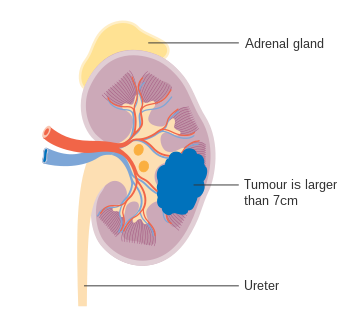
Tumor >7cm; limited to kidney
T2a, N0, M0
Tumor 7-≤10cm; limited to kidney
T2b, N0, M0
Tumor >10cm; limited to kidney
III
T3, N0, M0
Tumor extends to major veins or perinephric tissue but not into ipsilateral adrenal gland nor beyond Gerota's fascia
T3a, N0, M0
Tumor grossly extends into renal vein or its segmental branches, or tumor invades the pelvicalyceal system, or tumor invades perirenal and/or renal sinus fat but not beyond Gerota's fascia
T3b, N0, M0
Tumor grossly extends into vena cava below the diaphragm
T3c, N0, M0
Tumor grossly extends into vena cava above the diaphragm or invades the wall of the vena cava
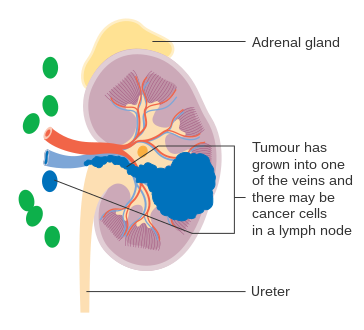
T1-T3, N1, M0
The main tumor can be any size and may be outside the kidney, but it has not spread beyond Gerota’s fascia. The cancer has spread to regional lymph nodes (N1) but has not spread to distant lymph nodes or other organs (M0).
IV
T4, any N, M0
Tumor invades beyond Gerota's fascia
Any T, any N, M1
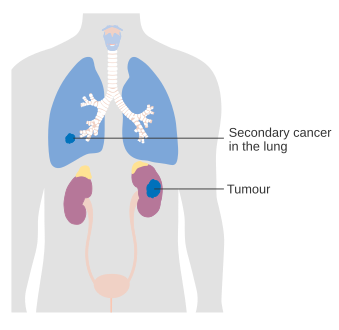
Tumor has spread to distant lymph nodes and/or other organs.
The lungs are the most common site for metastasis,[30] with other common sites including bone, brain, liver, adrenal gland and distant lymph nodes.[43][49][46]
Stage 1 kidney cancer
Stage 2 kidney cancer
Stage 3 kidney cancer
Stage 4 kidney cancer
Treatment
Treatment for kidney cancer depends on the type and stage of the disease. Surgery is the most common treatment as kidney cancer does not often respond to chemotherapy and radiotherapy. Surgical complexity can be estimated by the RENAL Nephrometry Scoring System. If the cancer has not spread it will usually be removed by surgery. In some cases this involves removing the whole kidney however most tumors are amenable to partial removal to eradicate the tumor and preserve the remaining normal portion of the kidney. Surgery is not always possible – for example, the patient may have other medical conditions that prevent it, or the cancer may have spread around the body and doctors may not be able to remove it.[50] If the cancer cannot be treated with surgery other techniques such as freezing the tumour or treating it with high temperatures may be used. However, these are not yet used as standard treatments for kidney cancer.[51] Recently, evidence stemming from the KEYNOTE-564 study has shed light on the potential use of systemic therapy in the adjuvant setting, with promising results. Patients exhibiting specific clear cell RCC tumor characteristics and having undergone treatment with Pembrolizumab for 17 cycles (around 1 year) had significant improvement in disease-free survival. However, the study has yet to yield conclusive findings in relation to overall survival. [52]
Other treatment options include biological therapies such as everolimus, torisel, nexavar, sutent, and axitinib, the use of immunotherapy including interferon and interleukin-2.[53][54][55] Immunotherapy is successful in 10 to 15% of people.[56]Sunitinib is the current standard of care in the adjuvant setting along with pazopanib; these treatments are often followed by everolimus, axitinib, and sorafenib. Immune checkpoint inhibitors are also in trials for kidney cancer, and some have gained approval for medical use.[57]
In the second line setting, nivolumab demonstrated an overall survival advantage in advanced clear renal cell carcinoma over everolimus in 2015 and was approved by the FDA.[57][58]Cabozantinib also demonstrated an overall survival benefit over everolimus and was approved by the FDA as a second-line treatment in 2016.[59][60][61]Lenvatinib in combination with everolimus was approved in 2016 for patients who have had exactly one prior line of angiogenic therapy.[62]
In Wilms' tumor, chemotherapy, radiotherapy and surgery are the accepted treatments, depending on the stage of the disease when it is diagnosed.[63]
Children
The majority of kidney cancers reported in children are Wilms' tumors. These tumors can begin to grow when a fetus is still developing in the uterus, and may not cause problems until the child is a few years old. Wilms' tumor is most common in children under the age of 5, but can rarely be diagnosed in older children or in adults. It is still not clear what causes most Wilms' tumors. The most common symptoms are swelling of the abdomen and blood in the urine.[63]
Epidemiology
Around 208,500 new cases of kidney cancer are diagnosed in the world each year, accounting for just under 2% of all cancers.[64] The highest rates are recorded in North America and the lowest rates in Asia and Africa.[65]
Lifestyle risk factors
Certain lifestyle factors have been associated with the development of renal cancer, although not all of them can be considered definitive causes. These include smoking, chemical carcinogens, radiation, viruses, diet and obesity, hypertension, diuretics,[14] and alcohol consumption.[12] Only a small percentage of kidney cancer cases have been linked to genetic factors.[12] With obesity listed as one of the risk factors, daily physical activity and engaging in a healthy diet is proven to lower the rates of developing kidney cancer in the future.[14]
Age
The incidence rate of renal cancer increases with the age of an individual, with 75 being the approximate age of the peak incidence rate, as of 2018.[12] However, nearly one half of all cases are diagnosed before the age of 65.[12] In both male and female children, renal tumors represent 2% to 6% of kidney cancer, with Wilms' tumor[14] being the most common.
Sex
The incidence of kidney cancer is two times greater in men than in women, and this is thought to be due to biological differences. Mortality rates typically decrease more rapidly in women compared to men.[12]
International variations
Incidence rates of kidney cancer can vary throughout the world. As of 2018, Czech Republic and Lithuania have the highest incidence rate of kidney cancer worldwide, with an age-standardized rate of 21.9/100,000 in males (Czech Republic) and 18.7/100,000 in males (Lithuania.) China, Thailand, and African countries (low-risk countries) have an incidence rate that is less than 2/100,000.[12]
Since the early 2000s, Austria and Poland have been the only countries to report a decrease in kidney cancer rates.[12]
Diagnosis access bias plays a large role in the epidemiology of kidney cancer. Differences in kidney cancer diagnosis across regions are likely due to differences in healthcare access, rather than a population's biological factors. Discrepancies in kidney cancer diagnosis has most likely led to the underrepresentation of mortality and incidence in low income countries.
Race
Race and ethnicity may be a factor in the distribution of kidney cancer around the United States. There are higher incidence rates in Black men and Hispanics, an average rate for American Indians, and low rates in Asians in the United States. Black people with kidney cancer have lower mortality rates than Caucasians in the United States.[12]
Screening
Accessibility for cancer screening is not very common due to high expenses. Improving cancer registries can improve care to those who have kidney cancer as well as decreasing the incidence and death rates. Safe and dependable treatment is key with the screening and treatment, which is not always the case in many developing nations.[66]
United States
The United States' NIH estimates for 2013 around 64,770 new cases of kidney cancer and 13,570 deaths from the disease.[67]
The incidence of kidney cancer is also increasing in the United States. This is thought to be a real increase, not only due to changes in the way the disease is diagnosed.[68]
Europe
The most recent estimates of incidence of kidney cancer suggest that there are 63,300 new cases annually in the EU25. In Europe, kidney cancer accounts for nearly 3% of all cancer cases.[69] Kidney cancer is the eighth most common cancer in the UK (around 10,100 people were diagnosed with the disease in 2011), and it is the fourteenth most common cause of cancer death (around 4,300 people died in 2012).[70]
Related Research Articles
Bladder cancer is any of several types of cancer arising from the tissues of the urinary bladder. Symptoms include blood in the urine, pain with urination, and low back pain. It is caused when epithelial cells that line the bladder become malignant.
Testicular cancer is cancer that develops in the testicles, a part of the male reproductive system. Symptoms may include a lump in the testicle or swelling or pain in the scrotum. Treatment may result in infertility.
Uterine cancer, also known as womb cancer, includes two types of cancer that develop from the tissues of the uterus. Endometrial cancer forms from the lining of the uterus, and uterine sarcoma forms from the muscles or support tissue of the uterus. Endometrial cancer accounts for approximately 90% of all uterine cancers in the United States. Symptoms of endometrial cancer include changes in vaginal bleeding or pain in the pelvis. Symptoms of uterine sarcoma include unusual vaginal bleeding or a mass in the vagina.
Renal cell carcinoma (RCC) is a kidney cancer that originates in the lining of the proximal convoluted tubule, a part of the very small tubes in the kidney that transport primary urine. RCC is the most common type of kidney cancer in adults, responsible for approximately 90–95% of cases. RCC occurrence shows a male predominance over women with a ratio of 1.5:1. RCC most commonly occurs between 6th and 7th decade of life.
Wilms' tumor or Wilms tumor, also known as nephroblastoma, is a cancer of the kidneys that typically occurs in children, and occurs most commonly as a renal tumor in child patients. It is named after Max Wilms, the German surgeon (1867–1918) who first described it.
A nephrectomy is the surgical removal of a kidney, performed to treat a number of kidney diseases including kidney cancer. It is also done to remove a normal healthy kidney from a living or deceased donor, which is part of a kidney transplant procedure.
Horseshoe kidney, also known as ren arcuatus, renal fusion or super kidney, is a congenital disorder affecting about 1 in 500 people that is more common in men, often asymptomatic, and usually diagnosed incidentally. In this disorder, the patient's kidneys fuse to form a horseshoe-shape during development in the womb. The fused part is the isthmus of the horseshoe kidney. The abnormal anatomy can affect kidney drainage resulting in increased frequency of kidney stones and urinary tract infections as well as increase risk of certain renal cancers.
Invasive carcinoma of no special type, invasive breast carcinoma of no special type (IBC-NST), invasive ductal carcinoma (IDC), infiltrating ductal carcinoma (IDC) or invasive ductal carcinoma, not otherwise specified (NOS) is a disease. For international audiences this article will use "invasive carcinoma NST" because it is the preferred term of the World Health Organization (WHO).
A blastoma is a type of cancer, more common in children, that is caused by malignancies in precursor cells, often called blasts. Examples are nephroblastoma, medulloblastoma, and retinoblastoma. The suffix -blastoma is used to imply a tumor of primitive, incompletely differentiated cells, e.g., chondroblastoma is composed of cells resembling the precursor of chondrocytes.
Sunitinib, sold under the brand name Sutent, is an anti-cancer medication. It is a small-molecule, multi-targeted receptor tyrosine kinase (RTK) inhibitor that was approved by the FDA for the treatment of renal cell carcinoma (RCC) and imatinib-resistant gastrointestinal stromal tumor (GIST) in January 2006. Sunitinib was the first cancer drug simultaneously approved for two different indications.
Transitional cell carcinoma, also called urothelial carcinoma, is a type of cancer that typically occurs in the urinary system. It is the most common type of bladder cancer and cancer of the ureter, urethra, and urachus. Symptoms of urothelial carcinoma in the bladder include hematuria. Diagnosis includes urine analysis and imaging of the urinary tract (cystoscopy). Transitional cell carcinomas arise from the transitional epithelium, a tissue lining the inner surface of these hollow organs. When the term "urothelial" is used, it specifically refers to a carcinoma of the urothelium, meaning a transitional cell carcinomas of the urinary system.
Vaginal cancer is an extraordinarily rare form of cancer that develops in the tissue of the vagina. Primary vaginal cancer originates from the vaginal tissue – most frequently squamous cell carcinoma, but primary vaginal adenocarcinoma, sarcoma, and melanoma have also been reported – while secondary vaginal cancer involves the metastasis of a cancer that originated in a different part of the body. Secondary vaginal cancer is more common. Signs of vaginal cancer may include abnormal vaginal bleeding, dysuria, tenesmus, or pelvic pain, though as many as 20% of women diagnosed with vaginal cancer are asymptomatic at the time of diagnosis. Vaginal cancer occurs more frequently in women over age 50, and the mean age of diagnosis of vaginal cancer is 60 years. It often can be cured if found and treated in early stages. Surgery alone or surgery combined with pelvic radiation is typically used to treat vaginal cancer.
Temsirolimus, sold under the brand name Torisel, is an intravenous drug for the treatment of renal cell carcinoma (RCC), developed by Wyeth Pharmaceuticals and approved by the U.S. Food and Drug Administration (FDA) in May 2007, and was also approved by the European Medicines Agency (EMA) in November 2007. It is a derivative and prodrug of sirolimus.
Congenital mesoblastic nephroma, while rare, is the most common kidney neoplasm diagnosed in the first three months of life and accounts for 3-5% of all childhood renal neoplasms. This neoplasm is generally non-aggressive and amenable to surgical removal. However, a readily identifiable subset of these kidney tumors has a more malignant potential and is capable of causing life-threatening metastases. Congenital mesoblastic nephroma was first named as such in 1967 but was recognized decades before this as fetal renal hamartoma or leiomyomatous renal hamartoma.
Urologic diseases or conditions include urinary tract infections, kidney stones, bladder control problems, and prostate problems, among others. Some urologic conditions do not affect a person for that long and some are lifetime conditions. Kidney diseases are normally investigated and treated by nephrologists, while the specialty of urology deals with problems in the other organs. Gynecologists may deal with problems of incontinence in women.
Renal medullary carcinoma is a rare type of cancer that affects the kidney. It tends to be aggressive, difficult to treat, and is often metastatic at the time of diagnosis. Most individuals with this type of cancer have sickle cell trait or rarely sickle cell disease, suggesting that the sickle cell trait may be a risk factor for this type of cancer.
Kidney tumours are tumours, or growths, on or in the kidney. These growths can be benign or malignant.
Ureteral cancer is cancer of the ureters, muscular tubes that propel urine from the kidneys to the urinary bladder. It is also known as ureter cancer, renal pelvic cancer, and rarely ureteric cancer or uretal cancer. Cancer in this location is rare. Ureteral cancer becomes more likely in older adults, usually ages 70–80, who have previously been diagnosed with bladder cancer.
Papillary renal cell carcinoma (PRCC) is a malignant, heterogeneous tumor originating from renal tubular epithelial cells of the kidney, which comprises approximately 10-15% of all kidney neoplasms. Based on its morphological features, PRCC can be classified into two main subtypes, which are type 1 (basophilic) and type 2 (eosinophilic).
Toni K. Choueiri is a Lebanese American medical oncologist and researcher. He is the Jerome and Nancy Kohlberg Professor of Medicine at Harvard Medical School and Director of the Lank Center for Genitourinary Oncology at the Dana–Farber Cancer Institute. His work has led to the establishment of several novel drugs and prognostic factors in advanced renal cell carcinoma (RCC). Choueiri also co-established the International metastatic database Consortium with Daniel Heng. His biomarker work has shed light on complex immunogenomics mechanisms contributing to response and resistance to targeted therapy and immunotherapy.
↑ "Kidney Cancer". National Cancer Institute. 2019. Retrieved 8 June 2019.
↑ Mulders PF, Brouwers AH, Hulsbergen-van der Kaa CA, van Lin EN, Osanto S, de Mulder PH (February 2008). "[Guideline 'Renal cell carcinoma']". Ned Tijdschr Geneeskd (in Dutch). 152 (7): 376–80. PMID18380384.
↑ Hidayat K, Du X, Zou SY, Shi BM (July 2017). "Blood pressure and kidney cancer risk: meta-analysis of prospective studies". Journal of Hypertension. 35 (7): 1333–1344. doi:10.1097/HJH.0000000000001286. PMID28157813. S2CID3454741.
↑ Kuroda N, Katto K, Tamura M, Shiotsu T, Hes O, Michal M, Nagashima Y, Ohara M, Hirouchi T, Mizuno K, Hayashi Y, Lee GH (January 2008). "Carcinoid tumor of the renal pelvis: consideration on the histogenesis". Pathol. Int. 58 (1): 51–4. doi:10.1111/j.1440-1827.2007.02188.x. PMID18067641. S2CID27645211.
↑ Picozzi S, Casellato S, Bozzini G, Ratti D, Macchi A, Rubino B, Pace G, Carmignani L (November 2013). "Inverted papilloma of the bladder: a review and an analysis of the recent literature of 365 patients". Urologic Oncology. 31 (8): 1584–1590. doi:10.1016/j.urolonc.2012.03.009. ISSN1873-2496. PMID22520573.
1 2 Syn NL, Teng MW, Mok TS, Soo RA (2017). "De-novo and acquired resistance to immune checkpoint targeting". The Lancet Oncology. 18 (12): e731–e741. doi:10.1016/s1470-2045(17)30607-1. PMID29208439.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.