Lung cancer, also known as lung carcinoma, is a malignant tumor that begins in the lung. Lung cancer is caused by genetic damage to the DNA of cells in the airways, often caused by cigarette smoking or inhaling damaging chemicals. Damaged airway cells gain the ability to multiply unchecked, causing the growth of a tumor. Without treatment, tumors spread throughout the lung, damaging lung function. Eventually lung tumors metastasize, spreading to other parts of the body.

A computed tomography scan is a medical imaging technique used to obtain detailed internal images of the body. The personnel that perform CT scans are called radiographers or radiology technologists.
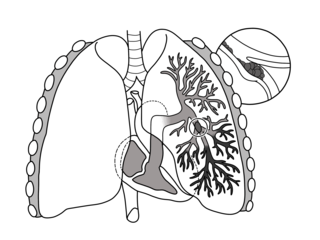
Pulmonary embolism (PE) is a blockage of an artery in the lungs by a substance that has moved from elsewhere in the body through the bloodstream (embolism). Symptoms of a PE may include shortness of breath, chest pain particularly upon breathing in, and coughing up blood. Symptoms of a blood clot in the leg may also be present, such as a red, warm, swollen, and painful leg. Signs of a PE include low blood oxygen levels, rapid breathing, rapid heart rate, and sometimes a mild fever. Severe cases can lead to passing out, abnormally low blood pressure, obstructive shock, and sudden death.

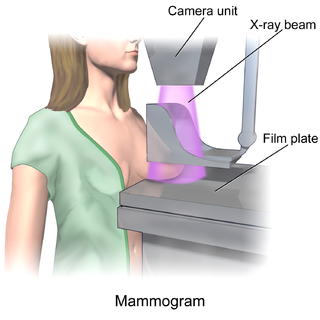
Mammography is the process of using low-energy X-rays to examine the human breast for diagnosis and screening. The goal of mammography is the early detection of breast cancer, typically through detection of characteristic masses or microcalcifications.
In medical or research imaging, an incidental imaging finding is an unanticipated finding which is not related to the original diagnostic inquiry. As with other types of incidental medical findings, they may represent a diagnostic, ethical, and philosophical dilemma because their significance is unclear. While some coincidental findings may lead to beneficial diagnoses, others may lead to overdiagnosis that results in unnecessary testing and treatment, sometimes called the "cascade effect".

Tuberculosis is diagnosed by finding Mycobacterium tuberculosis bacteria in a clinical specimen taken from the patient. While other investigations may strongly suggest tuberculosis as the diagnosis, they cannot confirm it.
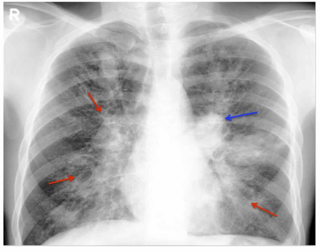
Community-acquired pneumonia (CAP) refers to pneumonia contracted by a person outside of the healthcare system. In contrast, hospital-acquired pneumonia (HAP) is seen in patients who have recently visited a hospital or who live in long-term care facilities. CAP is common, affecting people of all ages, and its symptoms occur as a result of oxygen-absorbing areas of the lung (alveoli) filling with fluid. This inhibits lung function, causing dyspnea, fever, chest pains and cough.
Allergic bronchopulmonary aspergillosis (ABPA) is a condition characterised by an exaggerated response of the immune system to the fungus Aspergillus. It occurs most often in people with asthma or cystic fibrosis. Aspergillus spores are ubiquitous in soil and are commonly found in the sputum of healthy individuals. A. fumigatus is responsible for a spectrum of lung diseases known as aspergilloses.

Computed tomography angiography is a computed tomography technique used for angiography—the visualization of arteries and veins—throughout the human body. Using contrast injected into the blood vessels, images are created to look for blockages, aneurysms, dissections, and stenosis. CTA can be used to visualize the vessels of the heart, the aorta and other large blood vessels, the lungs, the kidneys, the head and neck, and the arms and legs. CTA can also be used to localise arterial or venous bleed of the gastrointestinal system.

A CT pulmonary angiogram (CTPA) is a medical diagnostic test that employs computed tomography (CT) angiography to obtain an image of the pulmonary arteries. Its main use is to diagnose pulmonary embolism (PE). It is a preferred choice of imaging in the diagnosis of PE due to its minimally invasive nature for the patient, whose only requirement for the scan is an intravenous line.
A coronary CT calcium scan is a computed tomography (CT) scan of the heart for the assessment of severity of coronary artery disease. Specifically, it looks for calcium deposits in atherosclerotic plaques in the coronary arteries that can narrow arteries and increase the risk of heart attack. These plaques are the cause of most heart attacks, and become calcified as they develop.

Tomosynthesis, also digital tomosynthesis (DTS), is a method for performing high-resolution limited-angle tomography at radiation dose levels comparable with projectional radiography. It has been studied for a variety of clinical applications, including vascular imaging, dental imaging, orthopedic imaging, mammographic imaging, musculoskeletal imaging, and chest imaging.

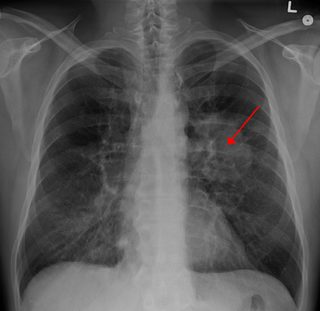
A lung nodule or pulmonary nodule is a relatively small focal density in the lung. A solitary pulmonary nodule (SPN) or coin lesion, is a mass in the lung smaller than three centimeters in diameter. A pulmonary micronodule has a diameter of less than three millimetres. There may also be multiple nodules.

The objective of cancer screening is to detect cancer before symptoms appear, involving various methods such as blood tests, urine tests, DNA tests, and medical imaging. The purpose of screening is early cancer detection, to make the cancer easier to treat and extending life expectancy. In 2019, cancer was the second leading cause of death globally; more recent data is pending due to the COVID-19 pandemic.

Adenocarcinoma of the lung is the most common type of lung cancer, and like other forms of lung cancer, it is characterized by distinct cellular and molecular features. It is classified as one of several non-small cell lung cancers (NSCLC), to distinguish it from small cell lung cancer which has a different behavior and prognosis. Lung adenocarcinoma is further classified into several subtypes and variants. The signs and symptoms of this specific type of lung cancer are similar to other forms of lung cancer, and patients most commonly complain of persistent cough and shortness of breath.
The National Lung Screening Trial was a United States-based clinical trial which recruited research participants between 2002 and 2004. It was sponsored by the National Cancer Institute and conducted by the American College of Radiology Imaging Network and the Lung Screening Study Group. The major objective of the trial was to compare the efficacy of low-dose helical computed tomography and standard chest X-ray as methods of lung cancer screening. The primary study ended in 2010, and the initial findings were published in November 2010, with the main results published in 2011 in the New England Journal of Medicine.
In medicine, breast imaging is a sub-speciality of diagnostic radiology that involves imaging of the breasts for screening or diagnostic purposes. There are various methods of breast imaging using a variety of technologies as described in detail below. Traditional screening and diagnostic mammography uses x-ray technology and has been the mainstay of breast imaging for many decades. Breast tomosynthesis is a relatively new digital x-ray mammography technique that produces multiple image slices of the breast similar to, but distinct from, computed tomography (CT). Xeromammography and galactography are somewhat outdated technologies that also use x-ray technology and are now used infrequently in the detection of breast cancer. Breast ultrasound is another technology employed in diagnosis and screening that can help differentiate between fluid filled and solid lesions, an important factor to determine if a lesion may be cancerous. Breast MRI is a technology typically reserved for high-risk patients and patients recently diagnosed with breast cancer. Lastly, scintimammography is used in a subgroup of patients who have abnormal mammograms or whose screening is not reliable on the basis of using traditional mammography or ultrasound.

Limited-stage small cell lung carcinoma (LS-SCLC) is a type of small cell lung cancer (SCLC) that is confined to an area which is small enough to be encompassed within a radiation portal. This generally includes cancer to one side of the lung and those might have reached the lymph nodes on the same side of the lung. 33% patients with small cell lung cancer are diagnosed with limited-stage small cell lung carcinoma when it is first found. Common symptoms include but are not limited to persistent cough, chest pain, rust-coloured sputum, shortness of breath, fatigue, weight loss, wheezing, hoarseness and recurrent respiratory tract infections such as pneumonia and bronchitis. Nervous system problems, Cushing syndrome and SIADH can also be associated with small cell lung cancer. Unlike extensive-stage small cell lung cancer, limited-stage small cell lung carcinoma is potentially curable. Standard treatments consist of surgery, platinum-based combination chemotherapy, thoracic irradiation, and prophylactic cranial irradiation. Patient five-year survival rate has significantly increased from 1% with surgery to 26% after the application of combination chemotherapy.
Denise R. Aberle is an American radiologist and oncologist. As a professor of radiology in the David Geffen School of Medicine at UCLA and a professor of bioengineering in the UCLA Henry Samueli School of Engineering and Applied Science, Aberle was elected a member of the National Academy of Medicine and Fellow of the American Institute for Medical and Biological Engineering.

Smoking-related interstitial fibrosis (SRIF) is an abnormality in the lungs characterized by excessive collagen deposition within the walls of the air sacs. This abnormality can be seen with a microscope and diagnosed by pathologists. It is caused by cigarette smoking.


