
Cancer is a group of diseases involving abnormal cell growth with the potential to invade or spread to other parts of the body. These contrast with benign tumors, which do not spread. Possible signs and symptoms include a lump, abnormal bleeding, prolonged cough, unexplained weight loss, and a change in bowel movements. While these symptoms may indicate cancer, they can also have other causes. Over 100 types of cancers affect humans.

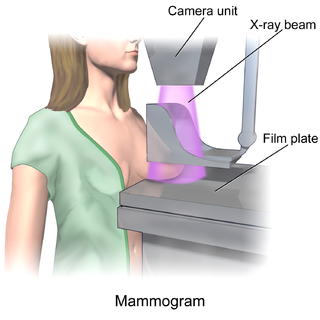
Mammography is the process of using low-energy X-rays to examine the human breast for diagnosis and screening. The goal of mammography is the early detection of breast cancer, typically through detection of characteristic masses or microcalcifications.

In a physical examination, medical examination, or clinical examination, a medical practitioner examines a patient for any possible medical signs or symptoms of a medical condition. It generally consists of a series of questions about the patient's medical history followed by an examination based on the reported symptoms. Together, the medical history and the physical examination help to determine a diagnosis and devise the treatment plan. These data then become part of the medical record.

Screening, in medicine, is a strategy used to look for as-yet-unrecognised conditions or risk markers. This testing can be applied to individuals or to a whole population without symptoms or signs of the disease being screened.
Canine cancer detection is an approach to cancer screening that relies upon the claimed olfactory ability of dogs to detect, in urine or in breath, very low concentrations of the alkanes and aromatic compounds generated by malignant tumors. While some research has been promising, no verified studies by secondary research groups have substantiated the validity of positive, conclusive results.
The five-year survival rate is a type of survival rate for estimating the prognosis of a particular disease, normally calculated from the point of diagnosis. Lead time bias from earlier diagnosis can affect interpretation of the five-year survival rate.

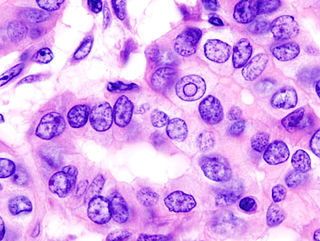
Ductal carcinoma in situ (DCIS), also known as intraductal carcinoma, is a pre-cancerous or non-invasive cancerous lesion of the breast. DCIS is classified as Stage 0. It rarely produces symptoms or a breast lump one can feel, typically being detected through screening mammography. It has been diagnosed in a significant percentage of men.
Breast cancer screening is the medical screening of asymptomatic, apparently healthy women for breast cancer in an attempt to achieve an earlier diagnosis. The assumption is that early detection will improve outcomes. A number of screening tests have been employed, including clinical and self breast exams, mammography, genetic screening, ultrasound, and magnetic resonance imaging.

The epidemiology of cancer is the study of the factors affecting cancer, as a way to infer possible trends and causes. The study of cancer epidemiology uses epidemiological methods to find the cause of cancer and to identify and develop improved treatments.
Thyroid cancer is cancer that develops from the tissues of the thyroid gland. It is a disease in which cells grow abnormally and have the potential to spread to other parts of the body. Symptoms can include swelling or a lump in the neck. Cancer can also occur in the thyroid after spread from other locations, in which case it is not classified as thyroid cancer.

The objective of cancer screening is to detect cancer before symptoms appear, involving various methods such as blood tests, urine tests, DNA tests, and medical imaging. The purpose of screening is early cancer detection, to make the cancer easier to treat and extending life expectancy. As of 2023, cancer is the second leading cause of death in the United States.
The PICO process is a mnemonic used in evidence-based practice to frame and answer a clinical or health care related question, though it is also argued that PICO "can be used universally for every scientific endeavour in any discipline with all study designs". The PICO framework is also used to develop literature search strategies, for instance in systematic reviews.
The mainstay of malaria diagnosis has been the microscopic examination of blood, utilizing blood films. Although blood is the sample most frequently used to make a diagnosis, both saliva and urine have been investigated as alternative, less invasive specimens. More recently, modern techniques utilizing antigen tests or polymerase chain reaction have been discovered, though these are not widely implemented in malaria endemic regions. Areas that cannot afford laboratory diagnostic tests often use only a history of subjective fever as the indication to treat for malaria.
Dynamic angiothermography (DATG) is a technique for the diagnosis of breast cancer. This technique, though springing from the previous conception of thermography, is based on a completely different principle. DATG records the temperature variations linked to the vascular changes in the breast due to angiogenesis. The presence, change, and growth of tumors and lesions in breast tissue change the vascular network in the breast. Consequently, through measuring the vascular structure over time, DATG effectively monitors the change in breast tissue due to tumors and lesions. It is currently used in combination with other techniques for diagnosis of breast cancer. This diagnostic method is a low-cost one compared with other techniques.
Overscreening, also called unnecessary screening, is the performance of medical screening without a medical indication to do so. Screening is a medical test in a healthy person who is showing no symptoms of a disease and is intended to detect a disease so that a person may prepare to respond to it. Screening is indicated in people who have some threshold risk for getting a disease, but is not indicated in people who are unlikely to develop a disease. Overscreening is a type of unnecessary health care.

H. Gilbert Welch is an American academic physician and cancer researcher. He was an internist at the Veterans Administration Medical Center in White River Junction, Vermont, as well as a professor of medicine at the Dartmouth Institute for Health Policy and Clinical Practice. In September 2018, Welch resigned from Dartmouth College after a 20-month long research misconduct investigation at Dartmouth concluded he had committed plagiarism.
The Canadian National Breast Screening Study, sometimes abbreviated as CNBSS or NBSS, was a randomized trial conducted with the aim of evaluating whether mammography reduced breast cancer incidence or mortality among women who underwent screening. The trial was initiated in 1980, and was conducted in fifteen screening centers in six different Canadian provinces. It was the first study designed to determine whether mammography was effective among women between the ages of 40 and 49.
In medicine, breast imaging is a sub-speciality of diagnostic radiology that involves imaging of the breasts for screening or diagnostic purposes. There are various methods of breast imaging using a variety of technologies as described in detail below. Traditional screening and diagnostic mammography uses x-ray technology and has been the mainstay of breast imaging for many decades. Breast tomosynthesis is a relatively new digital x-ray mammography technique that produces multiple image slices of the breast similar to, but distinct from, computed tomography (CT). Xeromammography and galactography are somewhat outdated technologies that also use x-ray technology and are now used infrequently in the detection of breast cancer. Breast ultrasound is another technology employed in diagnosis and screening that can help differentiate between fluid filled and solid lesions, an important factor to determine if a lesion may be cancerous. Breast MRI is a technology typically reserved for high-risk patients and patients recently diagnosed with breast cancer. Lastly, scintimammography is used in a subgroup of patients who have abnormal mammograms or whose screening is not reliable on the basis of using traditional mammography or ultrasound.
Jill Wruble is a radiologist and fellow at Johns Hopkins Medicine who is best known as a speaker on overdiagnosis due to incidental imaging finding in United States medicine.
Dense breast tissue, also known as dense breasts, is a condition of the breasts where a higher proportion of the breasts are made up of glandular tissue and fibrous tissue than fatty tissue. Around 40–50% of women have dense breast tissue and one of the main medical components of the condition is that mammograms are unable to differentiate tumorous tissue from the surrounding dense tissue. This increases the risk of late diagnosis of breast cancer in women with dense breast tissue. Additionally, women with such tissue have a higher likelihood of developing breast cancer in general, though the reasons for this are poorly understood.
