Related Research Articles
Suicide is the second leading cause of death for people in the United States from the ages of 10 to 56.
Suicide prevention is a collection of efforts to reduce the risk of suicide. Suicide is often preventable, and the efforts to prevent it may occur at the individual, relationship, community, and society level. Suicide is a serious public health problem that can have long-lasting effects on individuals, families, and communities. Preventing suicide requires strategies at all levels of society. This includes prevention and protective strategies for individuals, families, and communities. Suicide can be prevented by learning the warning signs, promoting prevention and resilience, and committing to social change.
Suicide intervention is a direct effort to prevent a person or persons from attempting to take their own life or lives intentionally.

Suicidal ideation, or suicidal thoughts, is the thought process of having ideas, or ruminations about the possibility of ending one's own life. It is not a diagnosis but is a symptom of some mental disorders and can also occur in response to adverse events without the presence of a mental disorder.
Suicide risk assessment is a process of estimating the likelihood for a person to attempt or die by suicide. The goal of a thorough risk assessment is to learn about the circumstances of an individual person with regard to suicide, including warning signs, risk factors, and protective factors. Risk for suicide is re-evaluated throughout the course of care to assess the patient's response to personal situational changes and clinical interventions. Accurate and defensible risk assessment requires a clinician to integrate a clinical judgment with the latest evidence-based practice, although accurate prediction of low base rate events, such as suicide, is inherently difficult and prone to false positives.
Youth suicide is when a young person, generally categorized as someone below the legal age of majority, deliberately ends their own life. Rates of youth suicide and attempted youth suicide in Western societies and other countries are high. Youth suicide attempts are more common among girls, but adolescent males are the ones who usually carry out suicide. Suicide rates in youths have nearly tripled between the 1960s and 1980s. For example, in Australia suicide is second only to motor vehicle accidents as its leading cause of death for people aged 15–25.
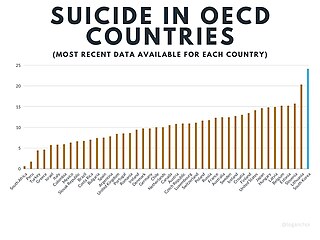
Suicide in South Korea occurs at the 12th highest rate in the world. South Korea has the highest recorded suicide rate in the OECD. However, differences in recording practices across the world make accurate comparisons impossible. In South Korea, it is estimated to affect 0.02 percent of the population by the WHO. In 2012, suicide was the fourth-highest cause of death. The suicide rate has consistently declined between 2012 and 2019, the year when the latest data is available.

Gender differences in suicide rates have been shown to be significant. There are different rates of suicides and suicidal behavior between males and females. While females more often have suicidal thoughts, males die by suicide more frequently. This discrepancy is also known as the gender paradox in suicide.
Research has found that attempted suicide rates and suicidal ideation among lesbian, gay, bisexual, transgender (LGBT) youth are significantly higher than among the general population.
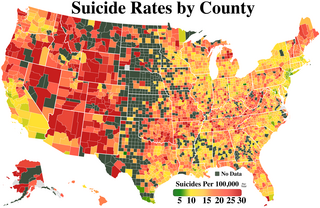
Suicide is a major national public health issue in the United States. The country has one of the highest suicide rates among wealthy nations. Since the beginning of 2023, there have been an average of about 67 suicide deaths per day in the United States. In 2020, there were 45,799 recorded suicides, up from 42,773 in 2014, according to the CDC's National Center for Health Statistics (NCHS). On average, adjusted for age, the annual U.S. suicide rate increased 30% between 2000 and 2020, from 10.4 to 13.5 suicides per 100,000 people. In 2018, 14.2 people per 100,000 died by suicide, the highest rate recorded in more than 30 years. Due to the stigma surrounding suicide, it is suspected that suicide is generally underreported. In April 2016, the CDC released data showing that the suicide rate in the United States had hit a 30-year high, and later in June 2018, released further data showing that the rate has continued to increase and has increased in every U.S. state except Nevada since 1999. From 2000 to 2020, more than 800,000 people died by suicide in the United States, with males representing 78.7% of all suicides that happened between 2000 and 2020. Surging death rates from suicide, drug overdoses and alcoholism, what researchers refer to as "deaths of despair", are largely responsible for a consecutive three year decline of life expectancy in the U.S. This constitutes the first three-year drop in life expectancy in the U.S. since the years 1915–1918.
A suicide attempt is an attempt to die by suicide that results in survival. It may be referred to as a "failed" or "unsuccessful" suicide attempt, though these terms are discouraged by mental health professionals for implying that a suicide resulting in death is a successful and positive outcome.
The relationship between antidepressant use and suicide risk is a subject of medical research and has faced varying levels of debate. This problem was thought to be serious enough to warrant intervention by the U.S. Food and Drug Administration to label greater likelihood of suicide as a risk of using antidepressants. Some studies have shown that the use of certain antidepressants correlate with an increased risk of suicide in some patients relative to other antidepressants. However, these conclusions have faced considerable scrutiny and disagreement: A multinational European study indicated that antidepressants decrease risk of suicide at the population level, and other reviews of antidepressant use claim that there is not enough data to indicate antidepressant use increases risk of suicide.

United States military veteran suicide is an ongoing phenomenon regarding the high rate of suicide among U.S. military veterans in comparison to the general civilian public. A focus on preventing veteran suicide began in 1958 with the opening of the first suicide prevention center in the United States. During the mid-1990s, a paradigm shift in addressing veteran suicide occurred with the development of a national strategy which included several Congressional Resolutions. More advancements were made in 2007, when the Joshua Omvig Veterans Suicide Prevention Act created a comprehensive program including outreach at each Veterans Affairs Office (VA) and the implementation of a 24-hour crisis hotline. PTSD, depression, and combat-related guilt in veterans are often related to suicide as it can be difficult for veterans to transition to civilian life.
In suicidology, psychological autopsy is a systematic procedure for evaluating suicidal intention in equivocal cases. It was invented by American psychologists Norman Farberow and Edwin S. Shneidman during their time working at the Los Angeles Suicide Prevention Center, which they founded in 1958.
In colleges and universities in the United States, suicide is one of the most common causes of death among students. Each year, approximately 24,000 college students attempt suicide while 1,100 students succeed in their attempt, making suicide the second-leading cause of death among U.S. college students. Roughly 12% of college students report the occurrence of suicide ideation during their first four years in college, with 2.6% percent reporting persistent suicide ideation. 65% of college students reported that they knew someone who has either attempted or died by suicide, showing that the majority of students on college campuses are exposed to suicide or suicidal attempts.
Suicide among Native Americans in the United States, both attempted and completed, is more prevalent than in any other racial or ethnic group in the United States. Among American youths specifically, Native American youths also show higher rates of suicide than American youths of other races. Despite making up only 0.9% of the total United States population, American Indians and Alaska Natives (AIANs) are a significantly heterogeneous group, with 560 federally recognized tribes, more than 200 non-federally recognized tribes, more than 300 languages spoken, and one half or more of them living in urban areas. Suicide rates are likewise variable within AIAN communities. Reported rates range from 0 to 150 per 100,000 members of the population for different groups. Native American men are more likely to commit suicide than Native American women, but Native American women show a higher prevalence of suicidal behaviors. Interpersonal relationships, community environment, spirituality, mental healthcare, and alcohol abuse interventions are among subjects of studies about the effectiveness of suicide prevention efforts. David Lester calls attention to the existence and importance of theories of suicide developed by indigenous peoples themselves, and notes that they "can challenge traditional Western theories of suicide." Studies by Olson and Wahab as well as Doll and Brady report that the Indian Health Service has lacked the resources needed to sufficiently address mental health problems in Native American communities. The most complete records of suicide among Native Americans in the United States are reported by the Indian Health Service.

The health access and health vulnerabilities experienced by the lesbian, gay, bisexual, transgender, queer or questioning, intersex, asexual (LGBTQIA) community in South Korea are influenced by the state's continuous failure to pass anti-discrimination laws that prohibit discrimination based on sexual orientation and gender identity. The construction and reinforcement of the South Korean national subject, "kungmin," and the basis of Confucianism and Christianity perpetuates heteronormativity, homophobia, discrimination, and harassment towards the LGBTQI community. The minority stress model can be used to explain the consequences of daily social stressors, like prejudice and discrimination, that sexual minorities face that result in a hostile social environment. Exposure to a hostile environment can lead to health disparities within the LGBTQI community, like higher rates of depression, suicide, suicide ideation, and health risk behavior. Korean public opinion and acceptance of the LGBTQI community have improved over the past two decades, but change has been slow, considering the increased opposition from Christian activist groups. In South Korea, obstacles to LGBTQI healthcare are characterized by discrimination, a lack of medical professionals and medical facilities trained to care for LGBTQI individuals, a lack of legal protection and regulation from governmental entities, and the lack of medical care coverage to provide for the health care needs of LGBTQI individuals. The presence of Korean LGBTQI organizations is a response to the lack of access to healthcare and human rights protection in South Korea. It is also important to note that research that focuses on Korean LGBTQI health access and vulnerabilities is limited in quantity and quality as pushback from the public and government continues.

Suicide cases have remained constant or decreased since the outbreak of the COVID-19 pandemic. According to a study done on twenty-one high and upper-middle-income countries in April–July 2020, the number of suicides has remained static. These results were attributed to a variety of factors, including the composition of mental health support, financial assistance, having families and communities work diligently to care for at-risk individuals, discovering new ways to connect through the use of technology, and having more time spent with family members which aided in the strengthening of their bonds. Despite this, there has been an increase in isolation, fear, stigma, abuse, and economic fallout as a result of COVID-19. Self-reported levels of depression, anxiety, and suicidal thoughts were elevated during the initial stay-at-home periods, according to empirical evidence from several countries, but this does not appear to have translated into an increase in suicides.
Douglas Alexander Mata is an American pathologist and epidemiologist currently at Foundation Medicine, Inc. in Cambridge, Massachusetts, known for his contributions to molecular pathological epidemiology and neuropsychiatric epidemiology. His textbook Statistics for Pathologists is a reference text in pathology medical education and his meta-analytical studies on physician mental health have circulated widely in the popular press.
Youth suicide in India is when young Indian people deliberately end their own life. People aged 15 to 24 years have the highest suicide rate in India, which is consistent with international trends in youth suicide. 35% of recorded suicides in India occur in this age group. Risk factors and methods of youth suicide differ from those in other age groups.
References
- ↑ Arnetz, B.B.; Hörte, L.G.; Hedberg, A.; Theorell, T.; Allander, E.; Malker, H. (1987). "Suicide patterns among physicians related to other academics as well as to the general population". Acta Psychiatrica Scandinavica. 75 (2): 139–143. doi:10.1111/j.1600-0447.1987.tb02765.x. ISSN 0001-690X.
- 1 2 Lindeman, S.; Laara, E.; Hakko, H.; Lonnqvist, J. (1996). "A systematic review on gender-specific suicide mortality in medical doctors". The British Journal of Psychiatry. 168 (3): 274–279. doi:10.1192/bjp.168.3.274. ISSN 0007-1250.
- ↑ "How Often do Physicians and Medical Students Die of Suicide". American Medical Association. Retrieved 17 July 2020.
- ↑ Schernhammer, Eva S.; Colditz, Graham A. (2004). "Suicide Rates Among Physicians: A Quantitative and Gender Assessment (Meta-Analysis)". American Journal of Psychiatry. 161 (12): 2295–2302. doi:10.1176/appi.ajp.161.12.2295. ISSN 0002-953X. PMID 15569903.
- ↑ Farmer, Blake (July 31, 2018). "When Doctors Struggle With Suicide, Their Profession Often Fails Them". NPR. Retrieved December 5, 2019.
- ↑ Tyssen, Reidar; Vaglum, Per; Grønvold, Nina T.; Ekeberg, Øivind (2001). "Suicidal ideation among medical students and young physicians: a nationwide and prospective study of prevalence and predictors". Journal of Affective Disorders. 64 (1): 69–79. doi:10.1016/S0165-0327(00)00205-6. ISSN 0165-0327.
- ↑ Yaghmour, Nicholas A.; Brigham, Timothy P.; Richter, Thomas; Miller, Rebecca S.; Philibert, Ingrid; Baldwin, DeWitt C.; Nasca, Thomas J. (July 2017). "Causes of Death of Residents in ACGME-Accredited Programs 2000 Through 2014". Academic Medicine. 92 (7): 976–983. doi:10.1097/ACM.0000000000001736. PMC 5483979 .
- ↑ Edwards, Ashley Alese (2 February 2018). "This NYC Hospital Has A Physician Suicide Problem It Doesn't Want You To Know About". Refinery29 .
- 1 2 Center, Claudia; Davis, Miriam; Detre, Thomas; Ford, Daniel E.; Hansbrough, Wendy; Hendin, Herbert; Laszlo, John; Litts, David A.; Mann, John; Mansky, Peter A.; Michels, Robert; Miles, Steven H.; Proujansky, Roy; Reynolds III, Charles F.; Silverman, Morton M. (2003). "Confronting Depression and Suicide in Physicians". JAMA. 289 (23): 3161. doi:10.1001/jama.289.23.3161. ISSN 0098-7484.
- ↑ American Foundation for Suicide Prevention. "Physician and Medical Student Depression and Suicide Prevention". American Foundation for Suicide Prevention. AFSP. Retrieved 16 September 2017.
- ↑ Do No Harm (2018) , retrieved 2017-06-19
- ↑ Watkins, Ali; Rothfeld, Michael; Rashbaum, William K.; Rosenthal, Brian M. (April 27, 2020). "Top E.R. Doctor Who Treated Virus Patients Dies by Suicide". The New York Times .
- ↑ Knoll, Corina; Watkins, Ali; Rothfeld, Michael (July 11, 2020). "'I Couldn't Do Anything': The Virus and an ER Doctor's Suicide". The New York Times .