An eating disorder is a mental disorder defined by abnormal eating behaviors that adversely affect a person's physical or mental health. Types of eating disorders include binge eating disorder, where the patient eats a large amount in a short period of time; anorexia nervosa, where the person has an intense fear of gaining weight and restricts food or overexercises to manage this fear; bulimia nervosa, where individuals eat a large quantity (binging) then try to rid themselves of the food (purging); pica, where the patient eats non-food items; rumination syndrome, where the patient regurgitates undigested or minimally digested food; avoidant/restrictive food intake disorder (ARFID), where people have a reduced or selective food intake due to some psychological reasons; and a group of other specified feeding or eating disorders. Anxiety disorders, depression and substance abuse are common among people with eating disorders. These disorders do not include obesity. People often experience comorbidity between an eating disorder and OCD. It is estimated 20–60% of patients with an ED have a history of OCD.

Bulimia nervosa, also known as simply bulimia, is an eating disorder characterized by binge eating followed by purging or fasting, and excessive concern with body shape and weight. This activity aims to expel the body of calories eaten from the binging phase of the process. Binge eating refers to eating a large amount of food in a short amount of time. Purging refers to the attempts to get rid of the food consumed. This may be done by vomiting or taking laxatives.

The enteric nervous system (ENS) or intrinsic nervous system is one of the main divisions of the peripheral nervous system (PNS) and consists of a mesh-like system of neurons that governs the function of the gastrointestinal tract. It is capable of acting independently of the sympathetic and parasympathetic nervous systems, although it may be influenced by them. The ENS is nicknamed the "second brain". It is derived from neural crest cells.
Orthorexia nervosa is a proposed eating disorder characterized by an excessive preoccupation with eating healthy food. The term was introduced in 1997 by American physician Steven Bratman, who suggested that some people's dietary restrictions intended to promote health may paradoxically lead to unhealthy consequences, such as social isolation, anxiety, loss of ability to eat in a natural, intuitive manner, reduced interest in the full range of other healthy human activities, and, in rare cases, severe malnutrition or even death.
Appetite is the desire to eat food items, usually due to hunger. Appealing foods can stimulate appetite even when hunger is absent, although appetite can be greatly reduced by satiety. Appetite exists in all higher life-forms, and serves to regulate adequate energy intake to maintain metabolic needs. It is regulated by a close interplay between the digestive tract, adipose tissue and the brain. Appetite has a relationship with every individual's behavior. Appetitive behaviour also known as approach behaviour, and consummatory behaviour, are the only processes that involve energy intake, whereas all other behaviours affect the release of energy. When stressed, appetite levels may increase and result in an increase of food intake. Decreased desire to eat is termed anorexia, while polyphagia is increased eating. Dysregulation of appetite contributes to anorexia nervosa, bulimia nervosa, cachexia, overeating, and binge eating disorder.
Binge eating disorder (BED) is an eating disorder characterized by frequent and recurrent binge eating episodes with associated negative psychological and social problems, but without the compensatory behaviors common to bulimia nervosa, OSFED, or the binge-purge subtype of anorexia nervosa.

Cachexia is a complex syndrome associated with an underlying illness, causing ongoing muscle loss that is not entirely reversed with nutritional supplementation. A range of diseases can cause cachexia, most commonly cancer, congestive heart failure, chronic obstructive pulmonary disease, chronic kidney disease, and AIDS. Systemic inflammation from these conditions can cause detrimental changes to metabolism and body composition. In contrast to weight loss from inadequate caloric intake, cachexia causes mostly muscle loss instead of fat loss. Diagnosis of cachexia can be difficult due to the lack of well-established diagnostic criteria. Cachexia can improve with treatment of the underlying illness but other treatment approaches have limited benefit. Cachexia is associated with increased mortality and poor quality of life.
Polyphagia or hyperphagia is an abnormally strong, incessant sensation of hunger or desire to eat often leading to overeating. In contrast to an increase in appetite following exercise, polyphagia does not subside after eating and often leads to rapid intake of excessive quantities of food. Polyphagia is not a disorder by itself; rather, it is a symptom indicating an underlying medical condition. It is frequently a result of abnormal blood glucose levels, and, along with polydipsia and polyuria, it is one of the "3 Ps" commonly associated with uncontrolled diabetes mellitus.

An underweight person is a person whose body weight is considered too low to be healthy. A person who is underweight is malnourished.

Relative energy deficiency in sport (RED-S) is a syndrome in which disordered eating, amenorrhoea/oligomenorrhoea, and decreased bone mineral density are present. It is caused by eating too little food to support the amount of energy being expended by an athlete, often at the urging of a coach or other authority figure who believes that athletes are more likely to win competitions when they have an extremely lean body type. RED-S is a serious illness with lifelong health consequences and can potentially be fatal.
Night eating syndrome (NES) is an eating disorder, characterized by a delayed circadian pattern of food intake. Although there is some degree of comorbidity with binge eating disorder, it differs from binge eating in that the amount of food consumed in the night is not necessarily objectively large nor is a loss of control over food intake required. It was originally described by Albert Stunkard in 1955 and is currently included in the other specified feeding or eating disorder category of the DSM-5. Research diagnostic criteria have been proposed and include evening hyperphagia and/or nocturnal awakening and ingestion of food two or more times per week. The person must have awareness of the night eating to differentiate it from the parasomnia sleep-related eating disorder (SRED). Three of five associated symptoms must also be present: lack of appetite in the morning, urges to eat at night, belief that one must eat in order to fall back to sleep at night, depressed mood, and/or difficulty sleeping.
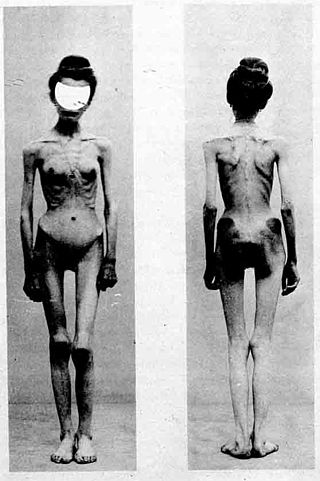
Some claim that the history of anorexia nervosa begins with descriptions of religious fasting dating from the Hellenistic era and continuing into the medieval period. A number of well known historical figures, including Catherine of Siena and Mary, Queen of Scots are believed to have suffered from the condition. Others link the emergence of anorexia to the distinctive presence of an extreme fear of being overweight despite being underweight which emerged in the second half of the 19th century and was first observed by Jean Martin Charcot and other French psychiatrists at the Salpetrière
Avoidant/restrictive food intake disorder (ARFID) is a feeding or eating disorder in which people avoid eating certain foods, or restrict their diets to the point it ultimately results in nutritional deficiencies. This can be due to the sensory characteristics of food, such as its appearance, smell, texture, or taste; due to fear of negative consequences such as choking or vomiting; having little interest in eating or food, or a combination of these factors. People with ARFID may also be afraid of trying new foods, a fear known as food neophobia.
Functional hypothalamic amenorrhea (FHA) is a form of amenorrhea and chronic anovulation and is one of the most common types of secondary amenorrhea. It is classified as hypogonadotropic hypogonadism. It was previously known as "juvenile hypothalamosis syndrome," prior to the discovery that sexually mature females are equally affected. FHA has multiple risk factors, with links to stress-related, weight-related, and exercise-related factors. FHA is caused by stress-induced suppression of the hypothalamic-pituitary-ovarian (HPO) axis, which results in inhibition of gonadotropin-releasing hormone (GnRH) secretion, and gonadotropins, follicle-stimulating hormone (FSH) and luteinizing hormone (LH). Severe and potentially prolonged hypoestrogenism is perhaps the most dangerous hormonal pathology associated with the disease, because consequences of this disturbance can influence bone health, cardiovascular health, mental health, and metabolic functioning in both the short and long-term. Because many of the symptoms overlap with those of organic hypothalamic, pituitary, or gonadal disease and therefore must be ruled out, FHA is a diagnosis of exclusion; "functional" is used to indicate a behavioral cause, in which no anatomical or organic disease is identified, and is reversible with correction of the underlying cause. Diagnostic workup includes a detailed history and physical, laboratory studies, such as a pregnancy test, and serum levels of FSH and LH, prolactin, and thyroid-stimulating hormone (TSH), and imaging. Additional tests may be indicated in order to distinguish FHA from organic hypothalamic or pituitary disorders. Patients present with a broad range of symptoms related to severe hypoestrogenism as well as hypercortisolemia, low serum insulin levels, low serum insulin-like growth factor 1 (IGF-1), and low total triiodothyronine (T3). Treatment is primarily managing the primary cause of the FHA with behavioral modifications. While hormonal-based therapies are potential treatment to restore menses, weight gain and behavioral modifications can have an even more potent impact on reversing neuroendocrine abnormalities, preventing further bone loss, and re-establishing menses, making this the recommended line of treatment. If this fails to work, secondary treatment is aimed at treating the effects of hypoestrogenism, hypercortisolism, and hypothyroidism.
An orexigenic, or appetite stimulant, is a drug, hormone, or compound that increases appetite and may induce hyperphagia. This can be a medication or a naturally occurring neuropeptide hormone, such as ghrelin, orexin or neuropeptide Y, which increases hunger and therefore enhances food consumption. Usually appetite enhancement is considered an undesirable side effect of certain drugs as it leads to unwanted weight gain, but sometimes it can be beneficial and a drug may be prescribed solely for this purpose, especially when the patient is suffering from severe appetite loss or muscle wasting due to cystic fibrosis, anorexia, old age, cancer or AIDS. There are several widely used drugs which can cause a boost in appetite, including tricyclic antidepressants (TCAs), tetracyclic antidepressants, natural or synthetic cannabinoids, first-generation antihistamines, most antipsychotics and many steroid hormones. In the United States, no hormone or drug has currently been approved by the FDA specifically as an orexigenic, with the exception of Dronabinol, which received approval for HIV/AIDS-induced anorexia only.

Anorexia nervosa (AN), often referred to simply as anorexia, is an eating disorder characterized by food restriction, body image disturbance, fear of gaining weight, and an overpowering desire to be thin.
The differential diagnoses of anorexia nervosa (AN) includes various types of medical and psychological conditions, which may be misdiagnosed as AN. In some cases, these conditions may be comorbid with AN because the misdiagnosis of AN is not uncommon. For example, a case of achalasia was misdiagnosed as AN and the patient spent two months confined to a psychiatric hospital. A reason for the differential diagnoses that surround AN arise mainly because, like other disorders, it is primarily, albeit defensively and adaptive for, the individual concerned. Anorexia Nervosa is a psychological disorder characterized by extremely reduced intake of food. People with anorexia nervosa tend to have a low self-image and an inaccurate perception of their body.

Many memory impairments exist as a result from or cause of eating disorders. Eating disorders (EDs) are characterized by abnormal and disturbed eating patterns that affect the lives of the individuals who worry about their weight to the extreme. These abnormal eating patterns involve either inadequate or excessive food intake, affecting the individual's physical and mental health.
Paul E. Garfinkel is a Canadian psychiatrist, researcher and an academic leader. He is a professor at the University of Toronto and a staff psychiatrist at Centre for Addiction and Mental Health (CAMH).
Atypical anorexia nervosa is an eating disorder in which individuals meet all the qualifications for anorexia nervosa, including a body image disturbance and a history of restrictive eating and weight loss, except that they are not currently underweight. Atypical anorexia qualifies as a mental health disorder in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), under the category Other Specified Feeding and Eating Disorders (OSFED). The characteristics of people with atypical anorexia generally do not differ significantly from anorexia nervosa patients except for their current weight.
