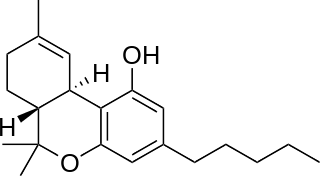
Tetrahydrocannabinol (THC) is the principal psychoactive constituent of cannabis and one of at least 113 total cannabinoids identified on the plant. Although the chemical formula for THC (C21H30O2) describes multiple isomers, the term THC usually refers to the delta-9-THC isomer with chemical name (−)-trans-Δ9-tetrahydrocannabinol. THC is a terpenoid found in cannabis and, like many pharmacologically active phytochemicals, it is assumed to be involved in the plant's evolutionary adaptation against insect predation, ultraviolet light, and environmental stress. THC was first discovered and isolated by Israeli chemist Raphael Mechoulam in Israel in 1964. It was found that, when smoked, THC is absorbed into the bloodstream and travels to the brain, attaching itself to endocannabinoid receptors located in the cerebral cortex, cerebellum, and basal ganglia. These are the parts of the brain responsible for thinking, memory, pleasure, coordination and movement.

The effects of cannabis are caused by chemical compounds in the cannabis plant, including 113 different cannabinoids such as tetrahydrocannabinol (THC) and 120 terpenes, which allow its drug to have various psychological and physiological effects on the human body. Different plants of the genus Cannabis contain different and often unpredictable concentrations of THC and other cannabinoids and hundreds of other molecules that have a pharmacological effect, so the final net effect cannot reliably be foreseen.

Medical cannabis, or medical marijuana (MMJ), is cannabis and cannabinoids that are prescribed by physicians for their patients. The use of cannabis as medicine has not been rigorously tested due to production and governmental restrictions, resulting in limited clinical research to define the safety and efficacy of using cannabis to treat diseases.
Cannabinoids are several structural classes of compounds found in the cannabis plant primarily and most animal organisms or as synthetic compounds. The most notable cannabinoid is the phytocannabinoid tetrahydrocannabinol (THC) (delta-9-THC), the primary psychoactive compound in cannabis. Cannabidiol (CBD) is also a major constituent of temperate cannabis plants and a minor constituent in tropical varieties. At least 113 distinct phytocannabinoids have been isolated from cannabis, although only four have been demonstrated to have a biogenetic origin. It was reported in 2020 that phytocannabinoids can be found in other plants such as rhododendron, licorice and liverwort, and earlier in Echinacea.
A drug test is a technical analysis of a biological specimen, for example urine, hair, blood, breath, sweat, or oral fluid/saliva—to determine the presence or absence of specified parent drugs or their metabolites. Major applications of drug testing include detection of the presence of performance enhancing steroids in sport, employers and parole/probation officers screening for drugs prohibited by law and police officers testing for the presence and concentration of alcohol (ethanol) in the blood commonly referred to as BAC. BAC tests are typically administered via a breathalyzer while urinalysis is used for the vast majority of drug testing in sports and the workplace. Numerous other methods with varying degrees of accuracy, sensitivity, and detection periods exist.

Cannabidiol (CBD) is a phytocannabinoid discovered in 1940. It is one of 113 identified cannabinoids in cannabis plants, along with tetrahydrocannabinol (THC), and accounts for up to 40% of the plant's extract. As of 2022, clinical research on CBD included studies related to the treatment of anxiety, addiction, psychosis, movement disorders, and pain, but there is insufficient high-quality evidence that cannabidiol is effective for these conditions. CBD is also sold as a herbal dietary supplement promoted with unproven claims of particular therapeutic effects.

Cannabis, also known as marijuana or weed among other names, is a psychoactive drug from the cannabis plant. Native to Central or South Asia, the cannabis plant has been used as a drug for both recreational and entheogenic purposes and in various traditional medicines for centuries. Tetrahydrocannabinol (THC) is the main psychoactive component of cannabis, which is one of the 483 known compounds in the plant, including at least 65 other cannabinoids, such as cannabidiol (CBD). Cannabis can be used by smoking, vaporizing, within food, or as an extract.
Enzyme multiplied immunoassay technique (EMIT) is a common method for qualitative and quantitative determination of therapeutic and recreational drugs and certain proteins in serum and urine.

11-Hydroxy-Δ9-tetrahydrocannabinol, usually referred to as 11-hydroxy-THC is the main active metabolite of tetrahydrocannabinol (THC), which is formed in the body after Δ9-THC is consumed.
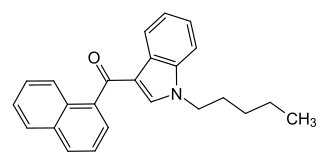
JWH-018 (1-pentyl-3-(1-naphthoyl)indole, NA-PIMO or AM-678) is an analgesic chemical from the naphthoylindole family that acts as a full agonist at both the CB1 and CB2 cannabinoid receptors, with some selectivity for CB2. It produces effects in animals similar to those of tetrahydrocannabinol (THC), a cannabinoid naturally present in cannabis, leading to its use in synthetic cannabis products that in some countries are sold legally as "incense blends".

11-Nor-9-carboxy-Δ9-tetrahydrocannabinol, often referred to as 11-nor-9-carboxy-THC or THC-11-oic acid, is the main secondary metabolite of tetrahydrocannabinol (THC) which is formed in the body after cannabis is consumed.

Synthetic cannabinoids are a class of designer drug molecules that bind to the same receptors to which cannabinoids in cannabis plants attach. These novel psychoactive substances should not be confused with synthetic phytocannabinoids or synthetic endocannabinoids from which they are in many aspects distinct.
The International Nonproprietary Name dronabinol, also known under the trade names Marinol and Syndros is a generic name for the molecule of delta-9-tetrahydrocannabinol in the pharmaceutical context. It has indications as an appetite stimulant, antiemetic, and sleep apnea reliever and is approved by the FDA as safe and effective for HIV/AIDS-induced anorexia and chemotherapy-induced nausea and vomiting only.

Tetrahydrocannabinolic acid is a precursor of tetrahydrocannabinol (THC), an active component of cannabis.
Two main questions arise in the law surrounding driving after having ingested cannabis: (1) whether cannabis actually impairs driving ability, and (2) whether the common practice of testing for THC is a reliable means to measure impairment. On the first question, studies are mixed. Several recent, extensive studies–including one conducted by the National Highway Traffic Safety Administration and one conducted by the American Automobile Association (AAA)–show that drivers with detectable THC in their blood are no more likely to cause car crashes than drivers with no amount of THC in their blood. Others show that cannabis can impair certain abilities important to safe driving –but no studies have been able to show that this increases the actual risk of crashing, or that drivers with THC in their blood cause a disproportionate number of crashes. On the second question, the studies that have been conducted so far have consistently found that THC blood levels and degree of impairment are not closely related. No known relationship between blood levels of THC and increased relative crash risk, or THC blood levels and level of driving impairment, has been shown by single-crash or classic-control studies. Thus, even though it is possible that cannabis impairs driving ability to some extent, there are currently no reliable means to test or measure whether a driver was actually impaired.
Occupational health concerns over the use of cannabis among workers are becoming increasingly important as cannabis becomes legal in more areas of the US. Of note, employers have concerns of workers either coming to work acutely impaired or recent use of cannabis still being detected in the body. Employment issues such as ADA law as it relates to accommodations for cannabis, paying unemployment benefits or paying out workers compensation benefits and disability claims are all important issues. While federal law still prohibits use, employers in different states have taken different stances based on whether they are federal contractors, perform safety sensitive work or whether the cannabis use is acutely impairing the employee.

Δ-8-tetrahydrocannabinol is a psychoactive cannabinoid found in the Cannabis plant. It is an isomer of delta-9-tetrahydrocannabinol, the compound commonly known as THC.

11-Hydroxy-Delta-8-tetrahydrocannabinol is an active metabolite of Δ8-THC, a psychoactive cannabinoid found in small amounts in cannabis. It is an isomer of 11-OH-Δ9-THC, and is produced via the same metabolic pathway. It was the first cannabinoid metabolite discovered in 1970.

Cannabitriol ((+)-CBT, (S,S)-9,10-Dihydroxy-Δ6a(10a)-THC) is a phytocannabinoid first isolated in 1966, an oxidation product of tetrahydrocannabinol which has been identified both as a trace component of cannabis and as a metabolite in cannabis users. Its pharmacology has been little studied, though it has been found to act as an antiestrogen and aromatase inhibitor.



