Alcohol intoxication, also known in overdose as alcohol poisoning, commonly described as drunkenness or inebriation, is the behavior and physical effects caused by a recent consumption of alcohol. In addition to the toxicity of ethanol, the main psychoactive component of alcoholic beverages, other physiological symptoms may arise from the activity of acetaldehyde, a metabolite of alcohol. These effects may not arise until hours after ingestion and may contribute to the condition colloquially known as a hangover. The term intoxication is commonly used when large amount of alcohol is consumed along with physical symptoms and deleterious health effects.
Glucose is a sugar with the molecular formula C6H12O6. Glucose is overall the most abundant monosaccharide, a subcategory of carbohydrates. Glucose is mainly made by plants and most algae during photosynthesis from water and carbon dioxide, using energy from sunlight, where it is used to make cellulose in cell walls, the most abundant carbohydrate in the world or, ATP(Adenosine Triphosphate) which is used by the cell as energy.

Uric acid is a heterocyclic compound of carbon, nitrogen, oxygen, and hydrogen with the formula C5H4N4O3. It forms ions and salts known as urates and acid urates, such as ammonium acid urate. Uric acid is a product of the metabolic breakdown of purine nucleotides, and it is a normal component of urine. High blood concentrations of uric acid can lead to gout and are associated with other medical conditions, including diabetes and the formation of ammonium acid urate kidney stones.

Alcohol by volume is a standard measure of how much alcohol is contained in a given volume of an alcoholic beverage. It is defined as the number of millilitres (mL) of pure ethanol present in 100 mL of solution at 20 °C (68 °F). The number of millilitres of pure ethanol is the mass of the ethanol divided by its density at 20 °C (68 °F), which is 0.78945 g/mL. The alc/vol standard is used worldwide. The International Organization of Legal Metrology has tables of density of water–ethanol mixtures at different concentrations and temperatures.
Hyperuricaemia or hyperuricemia is an abnormally high level of uric acid in the blood. In the pH conditions of body fluid, uric acid exists largely as urate, the ion form. Serum uric acid concentrations greater than 6 mg/dL for females, 7 mg/dL for men, and 5.5 mg/dL for youth are defined as hyperuricemia. The amount of urate in the body depends on the balance between the amount of purines eaten in food, the amount of urate synthesised within the body, and the amount of urate that is excreted in urine or through the gastrointestinal tract. Hyperuricemia may be the result of increased production of uric acid, decreased excretion of uric acid, or both increased production and reduced excretion.
Neotame, also known by the trade name Newtame, is a non-caloric artificial sweetener and aspartame analog by NutraSweet. By mass, it is 8000 times sweeter than sucrose. It has no notable off-flavors when compared to sucrose. It enhances original food flavors. It can be used alone, but is often mixed with other sweeteners to increase their individual sweetness and decrease their off-flavors. It is chemically somewhat more stable than aspartame. Its use can be cost effective in comparison to other sweeteners as smaller amounts of neotame are needed.

Forensic toxicology is a multidisciplinary field that combines the principles of toxicology with expertise in disciplines such as analytical chemistry, pharmacology and clinical chemistry to aid medical or legal investigation of death, poisoning, and drug use. The paramount focus for forensic toxicology is not the legal implications of the toxicological investigation or the methodologies employed, but rather the acquisition and accurate interpretation of results. Toxicological analyses can encompass a wide array of samples. In the course of an investigation, a forensic toxicologist must consider the context of an investigation, in particular any physical symptoms recorded, and any evidence collected at a crime scene that may narrow the search, such as pill bottles, powders, trace residue, and any available chemicals. Armed with this contextual information and samples to examine, the forensic toxicologist is tasked with identifying the specific toxic substances present, quantifying their concentrations, and assessing their likely impact on the individual involved.

A breathalyzer or breathalyser is a device for measuring breath alcohol content (BrAC). The name is a genericized trademark of the Breathalyzer brand name of instruments developed by inventor Robert Frank Borkenstein in the 1950s.

Fomepizole, also known as 4-methylpyrazole, is a medication used to treat methanol and ethylene glycol poisoning. It may be used alone or together with hemodialysis. It is given by injection into a vein.
Alcohol tolerance refers to the bodily responses to the functional effects of ethanol in alcoholic beverages. This includes direct tolerance, speed of recovery from insobriety and resistance to the development of alcohol use disorder.
Alcohol has a number of effects on health. Short-term effects of alcohol consumption include intoxication and dehydration. Long-term effects of alcohol include changes in the metabolism of the liver and brain, several types of cancer and alcohol use disorder. Alcohol intoxication affects the brain, causing slurred speech, clumsiness, and delayed reflexes. There is an increased risk of developing an alcohol use disorder for teenagers while their brain is still developing. Adolescents who drink have a higher probability of injury including death.
A hangover is the experience of various unpleasant physiological and psychological effects usually following the consumption of alcohol, such as wine, beer, and liquor. Hangovers can last for several hours or for more than 24 hours. Typical symptoms of a hangover may include headache, drowsiness, concentration problems, dry mouth, dizziness, fatigue, gastrointestinal distress, absence of hunger, light sensitivity, depression, sweating, hyper-excitability, irritability, and anxiety.

tert-Amyl alcohol (TAA) or 2-methylbutan-2-ol (2M2B), is a branched pentanol.

The short-term effects of alcohol consumption range from a decrease in anxiety and motor skills and euphoria at lower doses to intoxication (drunkenness), to stupor, unconsciousness, anterograde amnesia, and central nervous system depression at higher doses. Cell membranes are highly permeable to alcohol, so once it is in the bloodstream, it can diffuse into nearly every cell in the body.

Phosphatidylethanols (PEth) are a group of phospholipids formed only in the presence of ethanol via the action of phospholipase D (PLD). It accumulates in blood and is removed slowly, making it a useful biomarker for alcohol consumption. PEth is also thought to contribute to the symptoms of alcohol intoxication.

Drunk driving is the act of driving under the influence of alcohol. A small increase in the blood alcohol content increases the relative risk of a motor vehicle crash.
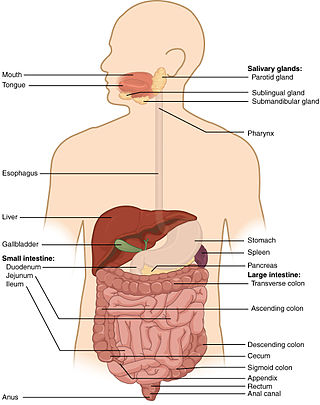
Auto-brewery syndrome(ABS) (also known as gut fermentation syndrome, endogenous ethanol fermentation or drunkenness disease) is a condition characterized by the fermentation of ingested carbohydrates in the gastrointestinal tract of the body caused by bacteria or fungi. ABS is a rare medical condition in which intoxicating quantities of ethanol are produced through endogenous fermentation within the digestive system. The organisms responsible for ABS include various yeasts and bacteria, including Saccharomyces cerevisiae, S. boulardii, Candida albicans, C. tropicalis, C. krusei, C. glabrata, C. kefyr, C. parapsilosis, Klebsiella pneumoniae, and Enterococcus faecium. These organisms use lactic acid fermentation or mixed acid fermentation pathways to produce an ethanol end product. The ethanol generated from these pathways is absorbed in the small intestine, causing an increase in blood alcohol concentrations that produce the effects of intoxication without the consumption of alcohol.

Methanol toxicity is poisoning from methanol, characteristically via ingestion. Symptoms may include a decreased level of consciousness, poor or no coordination, vomiting, abdominal pain, and a specific smell on the breath. Decreased vision may start as early as twelve hours after exposure. Long-term outcomes may include blindness and kidney failure. Blindness may occur after drinking as little as 10 mL; death may occur after drinking quantities over 15 mL.

Alcohol, sometimes referred to by the chemical name ethanol, is a depressant drug found in fermented beverages such as beer, wine, and distilled spirit — in particular, rectified spirit. Ethanol is colloquially referred to as "alcohol" because it is the most prevalent alcohol in alcoholic beverages, but technically all alcoholic beverages contain several types of psychoactive alcohols, that are categorized as primary, secondary, or tertiary; Primary, and secondary alcohols, are oxidized to aldehydes, and ketones, respectively, while tertiary alcohols are generally resistant to oxidation; Ethanol is a primary alcohol that has unpleasant actions in the body, many of which are mediated by its toxic metabolite acetaldehyde. Less prevalent alcohols found in alcoholic beverages, are secondary, and tertiary alcohols. For example, the tertiary alcohol 2M2B which is up to 50 times more potent than ethanol and found in trace quantities in alcoholic beverages, has been synthesized and used as a designer drug. Alcoholic beverages are sometimes laced with toxic alcohols, such as methanol and isopropyl alcohol. A mild, brief exposure to isopropyl alcohol is unlikely to cause any serious harm, but many methanol poisoning incidents have occurred through history, since methanol is lethal even in small quantities, as little as 10–15 milliliters. Ethanol is used to treat methanol and ethylene glycol toxicity.

N-Acetyltaurine (NAcT) is an endogenous metabolite. Biochemically, N-acetyltaurine is formed as a result of an acetylation of taurine. The main substrate for this reaction is acetate. An increase of endogenous N-acetyltaurine concentrations was observed after the consumption of alcohol and after extended physical activity (ketoacidosis).