Erectile dysfunction (ED), also referred to as impotence, is a form of sexual dysfunction in males characterized by the persistent or recurring inability to achieve or maintain a penile erection with sufficient rigidity and duration for satisfactory sexual activity. It is the most common sexual problem in males and can cause psychological distress due to its impact on self-image and sexual relationships.

Priapism is a condition in which a penis remains erect for hours in the absence of stimulation or after stimulation has ended. There are three types: ischemic (low-flow), nonischemic (high-flow), and recurrent ischemic (intermittent). Most cases are ischemic. Ischemic priapism is generally painful while nonischemic priapism is not. In ischemic priapism, most of the penis is hard; however, the glans penis is not. In nonischemic priapism, the entire penis is only somewhat hard. Very rarely, clitoral priapism occurs in women.
Erectile tissue is tissue in the body with numerous vascular spaces, or cavernous tissue, that may become engorged with blood. However, tissue that is devoid of or otherwise lacking erectile tissue may also be described as engorging with blood, often with regard to sexual arousal.

The corpus spongiosum is the mass of spongy tissue surrounding the male urethra within the penis. It is also called the corpus cavernosum urethrae in older texts.

The bulbospongiosus muscles are a subgroup of the superficial muscles of the perineum. They have a slightly different origin, insertion and function in males and females. In males, these muscles cover the bulb of the penis, while in females, they cover the vestibular bulbs.
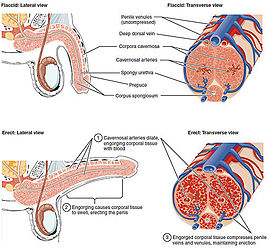
Tumescence is the quality or state of being tumescent or swollen. Tumescence usually refers to the normal engorgement with blood of the erectile tissues, marking sexual excitation, and possible readiness for sexual activity. The tumescent sexual organ in males is the penis and in females is the clitoris and other parts of the genitalia like the vestibular bulbs. Arteries in the penis dilate to increase blood volume.

A corpus cavernosum penis (singular) is one of a pair of sponge-like regions of erectile tissue, which contain most of the blood in the penis during an erection.
The dorsal artery of the penis is an artery on the top surface of the penis. It is a branch of the internal pudendal artery. It runs forward on the dorsum of the penis to the glans, where it divides into two branches to the glans penis and the foreskin (prepuce).

The corpus cavernosum of clitoris is one of a pair of sponge-like regions of erectile tissue of the clitoris. It is made of a sponge-like tissue that fills with blood during erection. This is homologous to the corpus cavernosum penis. The term corpora cavernosa literally means "cave-like bodies".
Nocturnal penile tumescence (NPT) is a spontaneous erection of the penis during sleep or when waking up. Along with nocturnal clitoral tumescence, it is also known as sleep-related erection. Men without physiological erectile dysfunction or severe depression experience nocturnal penile tumescence, usually three to five times during a period of sleep, typically during rapid eye movement sleep. Nocturnal penile tumescence is believed to contribute to penile health.
Venous leak, also called venogenic erectile dysfunction and penile venous insufficiency, is one category of vasculogenic impotence — a cause of erectile dysfunction in males. It affects all ages, being particularly awkward in young men. Much about venous leaks has not reached a consensus among the medical community, and many aspects of the condition, particularly its treatment strategies, are controversial. The prevalence of the condition is still unknown, although some sources claim it to be a common cause of erectile dysfunction.
The tunica albuginea is the fibrous envelope that extends the length of the corpora cavernosa penis and corpus spongiosum penis. It is a bi-layered structure that includes an outer longitudinal layer and an inner circular layer.

The helicine arteries of penis are arteries in the penis. They are found in the corpora cavernosa penis.

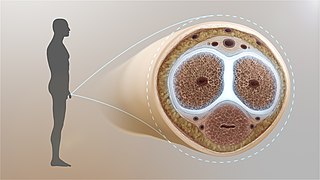
In human anatomy, the penis is an external male sex organ that additionally serves as the urinary duct. The main parts are the root, body, the epithelium of the penis including the shaft skin, and the foreskin covering the glans. The body of the penis is made up of three columns of tissue: two corpora cavernosa on the dorsal side and corpus spongiosum between them on the ventral side. The urethra passes through the prostate gland, where it is joined by the ejaculatory duct, and then through the penis. The urethra goes across the corpus spongiosum and ends at the tip of the glans as the opening, the urinary meatus. It is a passage both for excretion of urine and the ejaculation of semen.

The body or shaft of the penis is the free portion of the human penis that is located outside of the pelvic cavity. It is the continuation of the internal root, which is embedded in the pelvis and extends to the glans. It is made up of the two corpora cavernosa and the corpus spongiosum on the underside. The corpora cavernosa are intimately bound to one another with a dorsally fenestrated septum, which becomes a complete one before the penile crura. The body of the penis is homologous to the female clitoral body.

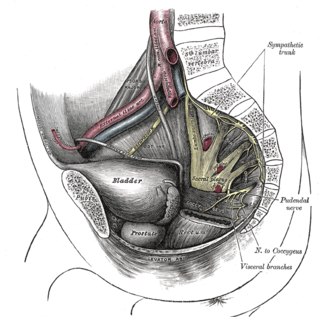
In human male anatomy, the radix or root of the penis is the internal and most proximal portion of the human penis that lies in the perineum. Unlike the pendulous body of the penis, which is suspended from the pubic symphysis, the root is attached to the pubic arch of the pelvis and is not visible externally. It is triradiate in form, consisting of three masses of erectile tissue; the two diverging crura, one on either side, and the median bulb of the penis or urethral bulb. Approximately one third to one half of the penis is embedded in the pelvis and can be felt through the scrotum and in the perineum.

Clitoral erection is a physiological phenomenon where the clitoris becomes enlarged and firm.
Penile ulltrasonography is medical ultrasonography of the penis. Ultrasound is an excellent method for the study of the penis, such as indicated in trauma, priapism, erectile dysfunction or suspected Peyronie's disease.
Hard flaccid syndrome (HFS), also known as hard flaccid (HF), is a chronic painful condition characterized by a semi-rigid penis at the flaccid state, a soft glans at the erect state (cold glans syndrome), pelvic pain, low libido, erectile dysfunction, erectile pain, pain on ejaculation, penile sensory changes (numbness or coldness), lower urinary tract symptoms, contraction of the pelvic floor muscles, and psychological distress. Other complaints include rectal and perineal discomfort, cold hands and feet, and a hollow or detached feeling inside the penile shaft. The majority of HFS patients are in their 20s–30s and symptoms significantly affect one's quality of life.

Glans insufficiency syndrome, also known as the soft glans, cold glans, or glans insufficiency, is a medical condition that affects male individuals. This condition is characterized by the persistent inability of the glans penis to achieve and maintain an erect or turgid state during sexual arousal, remaining soft and cold. This condition can have an impact on a person's sexual function, including decreased sensitivity, difficulty in maintaining an erection, and overall quality of life.









{kind=link}