
Otorhinolaryngology is a surgical subspeciality within medicine that deals with the surgical and medical management of conditions of the head and neck. Doctors who specialize in this area are called otorhinolaryngologists, otolaryngologists, head and neck surgeons, or ENT surgeons or physicians. Patients seek treatment from an otorhinolaryngologist for diseases of the ear, nose, throat, base of the skull, head, and neck. These commonly include functional diseases that affect the senses and activities of eating, drinking, speaking, breathing, swallowing, and hearing. In addition, ENT surgery encompasses the surgical management of cancers and benign tumors and reconstruction of the head and neck as well as plastic surgery of the face, scalp, and neck.
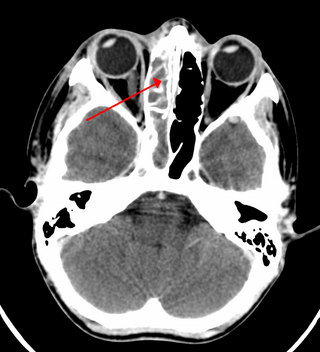
Sinusitis, also known as rhinosinusitis, is an inflammation of the mucous membranes that line the sinuses resulting in symptoms that may include thick nasal mucus, a plugged nose, and facial pain.

Otitis media is a group of inflammatory diseases of the middle ear. One of the two main types is acute otitis media (AOM), an infection of rapid onset that usually presents with ear pain. In young children this may result in pulling at the ear, increased crying, and poor sleep. Decreased eating and a fever may also be present. The other main type is otitis media with effusion (OME), typically not associated with symptoms, although occasionally a feeling of fullness is described; it is defined as the presence of non-infectious fluid in the middle ear which may persist for weeks or months often after an episode of acute otitis media. Chronic suppurative otitis media (CSOM) is middle ear inflammation that results in a perforated tympanic membrane with discharge from the ear for more than six weeks. It may be a complication of acute otitis media. Pain is rarely present. All three types of otitis media may be associated with hearing loss. If children with hearing loss due to OME do not learn sign language, it may affect their ability to learn.

Pharyngitis is inflammation of the back of the throat, known as the pharynx. It typically results in a sore throat and fever. Other symptoms may include a runny nose, cough, headache, difficulty swallowing, swollen lymph nodes, and a hoarse voice. Symptoms usually last 3–5 days, but can be longer depending on cause. Complications can include sinusitis and acute otitis media. Pharyngitis is a type of upper respiratory tract infection.

Laryngitis is inflammation of the larynx. Symptoms often include a hoarse voice and may include fever, cough, pain in the front of the neck, and trouble swallowing. Typically, these last under two weeks.

Conductive hearing loss (CHL) occurs when there is a problem transferring sound waves anywhere along the pathway through the outer ear, tympanic membrane (eardrum), or middle ear (ossicles). If a conductive hearing loss occurs in conjunction with a sensorineural hearing loss, it is referred to as a mixed hearing loss. Depending upon the severity and nature of the conductive loss, this type of hearing impairment can often be treated with surgical intervention or pharmaceuticals to partially or, in some cases, fully restore hearing acuity to within normal range. However, cases of permanent or chronic conductive hearing loss may require other treatment modalities such as hearing aid devices to improve detection of sound and speech perception.
Facial nerve paralysis is a common problem that involves the paralysis of any structures innervated by the facial nerve. The pathway of the facial nerve is long and relatively convoluted, so there are a number of causes that may result in facial nerve paralysis. The most common is Bell's palsy, a disease of unknown cause that may only be diagnosed by exclusion of identifiable serious causes.

Ear pain, also known as earache or otalgia, is pain in the ear. Primary ear pain is pain that originates from the ear. Secondary ear pain is a type of referred pain, meaning that the source of the pain differs from the location where the pain is felt.

Tympanostomy tube, also known as a grommet,myringotomy tube, or pressure equalizing tube, is a small tube inserted into the eardrum via a surgical procedure called myringotomy to keep the middle ear aerated for a prolonged period of time, typically to prevent accumulation of fluid in the middle ear. The tube itself is made in a variety of designs, most often shaped like a grommet for short-term use, or with long flanges and sometimes resembling a T-shape for long-term use. Materials used to manufacture the tubes are often made from fluoroplastic or silicone, which have largely replaced the use of metal tubes made from stainless steel, titanium, or gold.

Paronychia is an inflammation of the skin around the nail, which can occur suddenly, when it is usually due to the bacterium Staphylococcus aureus, or gradually when it is commonly caused by the fungus Candida albicans. The term is from Greek: παρωνυχία from para 'around', onyx 'nail', and the abstract noun suffix -ia.

Mastoiditis is the result of an infection that extends to the air cells of the skull behind the ear. Specifically, it is an inflammation of the mucosal lining of the mastoid antrum and mastoid air cell system inside the mastoid process. The mastoid process is the portion of the temporal bone of the skull that is behind the ear. The mastoid process contains open, air-containing spaces. Mastoiditis is usually caused by untreated acute otitis media and used to be a leading cause of child mortality. With the development of antibiotics, however, mastoiditis has become quite rare in developed countries where surgical treatment is now much less frequent and more conservative, unlike former times.
Otitis is a general term for inflammation in ear or ear infection, inner ear infection, middle ear infection of the ear, in both humans and other animals. When infection is present, it may be viral or bacterial. When inflammation is present due to fluid build up in the middle ear and infection is not present it is considered Otitis media with effusion. It is subdivided into the following:

A bone-anchored hearing aid (BAHA) is a type of hearing aid based on bone conduction. It is primarily suited for people who have conductive hearing losses, unilateral hearing loss, single-sided deafness and people with mixed hearing losses who cannot otherwise wear 'in the ear' or 'behind the ear' hearing aids. They are more expensive than conventional hearing aids, and their placement involves invasive surgery which carries a risk of complications, although when complications do occur, they are usually minor.

Surfer's ear is the common name for an exostosis or abnormal bone growth within the ear canal. They are otherwise benign hyperplasias (growths) of the tympanic bone thought to be caused by frequent cold-water exposure. Cases are often asymptomatic. Surfer's ear is not the same as swimmer's ear, although infection can result as a side effect.

Ear drops are a form of topical medication for the ears used to treat infection, inflammation, impacted ear wax and local anesthesia. They are commonly used for short-term treatment and can be purchased with or without a prescription. Before using ear drops, refer to the package insert or consult a health professional for the amount of drops to use and the duration of treatment.

Otitis externa is an inflammation of the outer ear and ear canal. Animals are commonly prone to ear infection, and this is one of the most common manifestations of allergy in dogs. In dogs, those breeds with floppy ears are more prone, since air flow is limited and a warm, moist environment built up, which is conducive to infection. The external ear in animals is longer and deeper than in humans, which makes it easier for infection or wax to build up or be hard to remove. Complete ear canal inspection requires the use of an otoscope by a veterinarian.
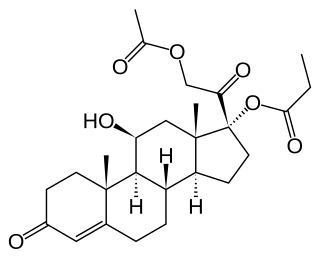
Hydrocortisone aceponate is a veterinary corticosteroid that is used in form of creams for the treatment of various dermatoses. It is an ester of hydrocortisone (cortisol) with acetic acid and propionic acid.
Otomycosis is a fungal ear infection, a superficial mycotic infection of the outer ear canal caused by micro-organisms called fungi which are related to yeast and mushrooms. It is more common in tropical or warm countries. The infection may be either subacute or acute and is characterized by itching in the ear, malodorous discharge, inflammation, pruritus, scaling, and severe discomfort or ear pain. The mycosis results in inflammation, superficial epithelial exfoliation, masses of debris containing hyphae, suppuration, and pain. Otomycosis can also cause hearing loss.

Finafloxacin (Xtoro) is a fluoroquinolone antibiotic. In the United States, it is approved by the Food and Drug Administration to treat acute otitis externa caused by the bacteria Pseudomonas aeruginosa and Staphylococcus aureus.
Granular myringitis is a long term condition in which there is inflammation of the tympanic membrane in the ear and formation of granulation tissue within the tympanic membrane. It is a type of otitis externa.


