Defecation follows digestion, and is a necessary process by which organisms eliminate a solid, semisolid, or liquid waste material known as feces from the digestive tract via the anus. The act has a variety of names ranging from the common, like pooping or crapping, to the technical, e.g. bowel movement, to the obscene (shitting), to the euphemistic, to the juvenile. The topic, usually avoided in polite company, can become the basis for some potty humor.

Fecal incontinence (FI), or in some forms encopresis, is a lack of control over defecation, leading to involuntary loss of bowel contents, both liquid stool elements and mucus, or solid feces. When this loss includes flatus (gas), it is referred to as anal incontinence. FI is a sign or a symptom, not a diagnosis. Incontinence can result from different causes and might occur with either constipation or diarrhea. Continence is maintained by several interrelated factors, including the anal sampling mechanism, and incontinence usually results from a deficiency of multiple mechanisms. The most common causes are thought to be immediate or delayed damage from childbirth, complications from prior anorectal surgery, altered bowel habits. An estimated 2.2% of community-dwelling adults are affected. However, reported prevalence figures vary. A prevalence of 8.39% among non-institutionalized U.S adults between 2005 and 2010 has been reported, and among institutionalized elders figures come close to 50%.
In anatomy, a fistula is an abnormal connection joining two hollow spaces, such as blood vessels, intestines, or other hollow organs to each other, often resulting in an abnormal flow of fluid from one space to the other. An anal fistula connects the anal canal to the perianal skin. An anovaginal or rectovaginal fistula is a hole joining the anus or rectum to the vagina. A colovaginal fistula joins the space in the colon to that in the vagina. A urinary tract fistula is an abnormal opening in the urinary tract or an abnormal connection between the urinary tract and another organ. An abnormal communication between the bladder and the uterus is called a vesicouterine fistula, while if it is between the bladder and the vagina it is known as a vesicovaginal fistula, and if between the urethra and the vagina: a urethrovaginal fistula. When occurring between two parts of the intestine, it is known as an enteroenteral fistula, between the small intestine and the skin as an enterocutaneous fistula, and between the colon and the skin as a colocutaneous fistula.
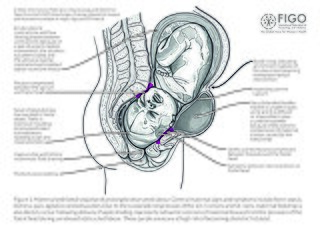
Obstetric fistula is a medical condition in which a hole develops in the birth canal as a result of childbirth. This can be between the vagina and rectum, ureter, or bladder. It can result in incontinence of urine or feces. Complications may include depression, infertility, and social isolation.

Lymphogranuloma venereum is a sexually transmitted infection caused by the invasive serovars L1, L2, L2a, L2b, or L3 of Chlamydia trachomatis.
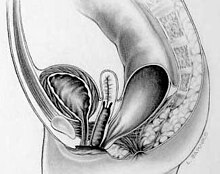
In gynecology, a rectocele or posterior vaginal wall prolapse results when the rectum bulges (herniates) into the vagina. Two common causes of this defect are childbirth and hysterectomy. Rectocele also tends to occur with other forms of pelvic organ prolapse, such as enterocele, sigmoidocele and cystocele.
In medicine, the ileal pouch–anal anastomosis (IPAA), also known as restorative proctocolectomy (RPC), ileal-anal reservoir (IAR), an ileo-anal pouch, ileal-anal pullthrough, or sometimes referred to as a J-pouch, S-pouch, W-pouch, or a pelvic pouch, is an anastomosis of a reservoir pouch made from ileum to the anus, bypassing the former site of the colon in cases where the colon and rectum have been removed. The pouch retains and restores functionality of the anus, with stools passed under voluntary control of the person, preventing fecal incontinence and serving as an alternative to a total proctocolectomy with ileostomy.
Proctitis is an inflammation of the anus and the lining of the rectum, affecting only the last 6 inches of the rectum.
Anal fistula is a chronic abnormal communication between the anal canal and the perianal skin. An anal fistula can be described as a narrow tunnel with its internal opening in the anal canal and its external opening in the skin near the anus. Anal fistulae commonly occur in people with a history of anal abscesses. They can form when anal abscesses do not heal properly.

Anorectal abscess is an abscess adjacent to the anus. Most cases of perianal abscesses are sporadic, though there are certain situations which elevate the risk for developing the disease, such as diabetes mellitus, Crohn's disease, chronic corticosteroid treatment and others. It arises as a complication of paraproctitis. Ischiorectal, inter- and intrasphincteric abscesses have been described.
Vaginal flatulence or vaginal wind is an emission or expulsion of air from the vagina. It may occur during or after sexual intercourse or during other sexual acts, stretching or exercise. The sound is often comparable to flatulence from the anus, but does not involve waste gases, and thus often does not have a specific odor associated. Slang terms for vaginal flatulence include queef, vart, and fanny fart. Tampons can treat or prevent vaginal wind.

In humans, the anus is the external opening of the rectum located inside the intergluteal cleft. Two sphincters control the exit of feces from the body during an act of defecation, which is the primary function of the anus. These are the internal anal sphincter and the external anal sphincter, which are circular muscles that normally maintain constriction of the orifice and which relaxes as required by normal physiological functioning. The inner sphincter is involuntary and the outer is voluntary. Above the anus is the perineum, which is also located beneath the vulva or scrotum.

A perineal tear is a laceration of the skin and other soft tissue structures which, in women, separate the vagina from the anus. Perineal tears mainly occur in women as a result of vaginal childbirth, which strains the perineum. It is the most common form of obstetric injury. Tears vary widely in severity. The majority are superficial and may require no treatment, but severe tears can cause significant bleeding, long-term pain or dysfunction. A perineal tear is distinct from an episiotomy, in which the perineum is intentionally incised to facilitate delivery. Episiotomy, a very rapid birth, or large fetal size can lead to more severe tears which may require surgical intervention.
Rectal discharge is intermittent or continuous expression of liquid from the anus. Normal rectal mucus is needed for proper excretion of waste. Otherwise, this is closely related to types of fecal incontinence but the term rectal discharge does not necessarily imply degrees of incontinence. Types of fecal incontinence that produce a liquid leakage could be thought of as a type of rectal discharge.
Obstructed defecation syndrome is a major cause of functional constipation, of which it is considered a subtype. It is characterized by difficult and/or incomplete emptying of the rectum with or without an actual reduction in the number of bowel movements per week. Normal definitions of functional constipation include infrequent bowel movements and hard stools. In contrast, ODS may occur with frequent bowel movements and even with soft stools, and the colonic transit time may be normal, but delayed in the rectum and sigmoid colon.
Fistulectomy is a surgical procedure where a surgeon completely removes a fistula, an abnormal tract that connects two hollow spaces of the body. In comparison to other procedural options of treating fistulae such as fistulotomies, where a fistula is cut open but not completely removed, and seton placement, where a rubber band seton is passed through the tract and left post-operation as a means to allow drainage of the fistula, fistulectomies are considered to be a more radical approach. The total removal of a fistula may damage nearby structures in the process.
A rectovestibular fistula, also referred to simply as a vestibular fistula, is an anorectal congenital disorder where an abnormal connection (fistula) exists between the rectum and the vulval vestibule of the female genitalia.
A urogenital fistula is an abnormal tract that exists between the urinary tract and bladder, ureters, or urethra. A urogenital fistula can occur between any of the organs and structures of the pelvic region. A fistula allows urine to continually exit through and out the urogenital tract. This can result in significant disability, interference with sexual activity, and other physical health issues, the effects of which may in turn have a negative impact on mental or emotional state, including an increase in social isolation. Urogenital fistulas vary in etiology. Fistulas are usually caused by injury or surgery, but they can also result from malignancy, infection, prolonged and obstructed labor and deliver in childbirth, hysterectomy, radiation therapy or inflammation. Of the fistulas that develop from difficult childbirth, 97 percent occur in developing countries. Congenital urogenital fistulas are rare; only ten cases have been documented. Abnormal passageways can also exist between the vagina and the organs of the gastrointestinal system, and these may also be termed fistulas.
Crohn's disease (CD) of the vulva is a rare extra intestinal condition, with granulomatous cutaneous lesions affecting the female genitalia. Lesions connected to the affected gut via a healthy tissue are referred to as metastatic lesions.
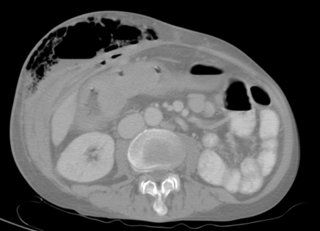
Pelvic abscess is a collection of pus in the pelvis, typically occurring following lower abdominal surgical procedures, or as a complication of pelvic inflammatory disease (PID), appendicitis, or lower genital tract infections. Signs and symptoms include a high fever, pelvic mass, vaginal bleeding or discharge, and lower abdominal pain. It can lead to sepsis and death.