Yellow fever is a viral disease of typically short duration. In most cases, symptoms include fever, chills, loss of appetite, nausea, muscle pains – particularly in the back – and headaches. Symptoms typically improve within five days. In about 15% of people, within a day of improving the fever comes back, abdominal pain occurs, and liver damage begins causing yellow skin. If this occurs, the risk of bleeding and kidney problems is increased.

Measles is a highly contagious, vaccine-preventable infectious disease caused by measles virus. Symptoms usually develop 10–12 days after exposure to an infected person and last 7–10 days. Initial symptoms typically include fever, often greater than 40 °C (104 °F), cough, runny nose, and inflamed eyes. Small white spots known as Koplik's spots may form inside the mouth two or three days after the start of symptoms. A red, flat rash which usually starts on the face and then spreads to the rest of the body typically begins three to five days after the start of symptoms. Common complications include diarrhea, middle ear infection (7%), and pneumonia (6%). These occur in part due to measles-induced immunosuppression. Less commonly seizures, blindness, or inflammation of the brain may occur. Other names include morbilli, rubeola, red measles, and English measles. Both rubella, also known as German measles, and roseola are different diseases caused by unrelated viruses.

Polio vaccines are vaccines used to prevent poliomyelitis (polio). Two types are used: an inactivated poliovirus given by injection (IPV) and a weakened poliovirus given by mouth (OPV). The World Health Organization (WHO) recommends all children be fully vaccinated against polio. The two vaccines have eliminated polio from most of the world, and reduced the number of cases reported each year from an estimated 350,000 in 1988 to 33 in 2018.

Crimean–Congo hemorrhagic fever (CCHF) is a viral disease. Symptoms of CCHF may include fever, muscle pains, headache, vomiting, diarrhea, and bleeding into the skin. Onset of symptoms is less than two weeks following exposure. Complications may include liver failure. Survivors generally recover around two weeks after onset.

Disease surveillance is an epidemiological practice by which the spread of disease is monitored in order to establish patterns of progression. The main role of disease surveillance is to predict, observe, and minimize the harm caused by outbreak, epidemic, and pandemic situations, as well as increase knowledge about which factors contribute to such circumstances. A key part of modern disease surveillance is the practice of disease case reporting.

Polio eradication, the permanent global cessation of circulation of the poliovirus and hence elimination of the poliomyelitis (polio) it causes, is the aim of a multinational public health effort begun in 1988, led by the World Health Organization (WHO), the United Nations Children's Fund (UNICEF) and the Rotary Foundation. These organizations, along with the U.S. Centers for Disease Control and Prevention (CDC) and The Gates Foundation, have spearheaded the campaign through the Global Polio Eradication Initiative (GPEI). Successful eradication of infectious diseases has been achieved twice before, with smallpox in humans and rinderpest in ruminants.

Program for Monitoring Emerging Diseases is among the largest publicly available emerging diseases and outbreak reporting systems in the world. The purpose of ProMED is to promote communication amongst the international infectious disease community, including scientists, physicians, veterinarians, epidemiologists, public health professionals, and others interested in infectious diseases on a global scale. Founded in 1994, ProMED has pioneered the concept of electronic, Internet-based emerging disease and outbreak detection reporting. In 1999, ProMED became a program of the International Society for Infectious Diseases. As of 2016, ProMED has more than 75,000 subscribers in over 185 countries. With an average of 13 posts per day, ProMED provides users with up-to-date information concerning infectious disease outbreaks on a global scale.

Measles vaccine protects against becoming infected with measles. Nearly all of those who do not develop immunity after a single dose develop it after a second dose. When rate of vaccination within a population is greater than 92%, outbreaks of measles typically no longer occur; however, they may occur again if the rate of vaccination decrease. The vaccine's effectiveness lasts many years. It is unclear if it becomes less effective over time. The vaccine may also protect against measles if given within a couple of days after exposure to measles.

Yellow fever vaccine is a vaccine that protects against yellow fever. Yellow fever is a viral infection that occurs in Africa and South America. Most people begin to develop immunity within ten days of vaccination and 99% are protected within one month, and this appears to be lifelong. The vaccine can be used to control outbreaks of disease. It is given either by injection into a muscle or just under the skin.

Recombinant vesicular stomatitis virus–Zaire Ebola virus (rVSV-ZEBOV), also known as Ebola Zaire vaccine live and sold under the brand name Ervebo, is an Ebola vaccine for adults that prevents Ebola caused by the Zaire ebolavirus. When used in ring vaccination, rVSV-ZEBOV has shown a high level of protection. Around half the people given the vaccine have mild to moderate adverse effects that include headache, fatigue, and muscle pain.
In late 2012, a yellow fever outbreak occurred in the Darfur region of Sudan that was the largest yellow fever epidemic to strike Africa in two decades. On 10 January 2013, the Sudan Federal Ministry of Health and the World Health Organization (WHO) reported that there had been 847 suspected cases since 2 September 2012, including 171 deaths, for an estimated case fatality rate of 20%. A mass vaccination campaign was launched in mid-November. By early January, the five states of Darfur were free of any new cases.

John Payne Woodall (1935–2016), known as Jack Woodall, was an American-British entomologist and virologist who made significant contributions to the study of arboviruses in South America, the Caribbean and Africa. He did research on the causative agents of dengue fever, Crimean–Congo hemorrhagic fever, o'nyong'nyong fever, yellow fever, Zika fever, and others.

The Democratic Republic of the Congo (DRC) was identified by the World Health Organization (WHO) on 11 May 2017 as having one Ebola-related death.

The 2018 Équateur province Ebola outbreak occurred in the north-west of the Democratic Republic of the Congo (DRC) from May to July 2018. It was contained entirely within Équateur province, and was the first time that vaccination with the rVSV-ZEBOV Ebola vaccine had been attempted in the early stages of an Ebola outbreak, with a total of 3,481 people vaccinated. It was the ninth recorded Ebola outbreak in the DRC.

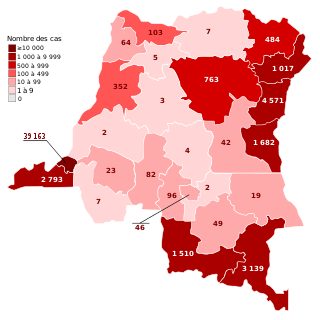
The Kivu Ebola epidemic was an outbreak of Ebola virus disease (EVD) mainly in eastern Democratic Republic of the Congo (DRC), and in other parts of Central Africa, from 2018 to 2020. Between 1 August 2018 and 25 June 2020 it resulted in 3,470 reported cases. The Kivu outbreak also affected Ituri Province, whose first case was confirmed on 13 August 2018. In November 2018, the outbreak became the biggest Ebola outbreak in the DRC's history, and had become the second-largest Ebola outbreak in recorded history worldwide, behind only the 2013–2016 Western Africa epidemic. In June 2019, the virus reached Uganda, having infected a 5-year-old Congolese boy who entered Uganda with his family, but was contained.
Daniel R. Lucey is an American physician, researcher, senior scholar and adjunct professor of infectious diseases at Georgetown University, and a research associate in anthropology at the Smithsonian National Museum of Natural History, where he has co-organised an exhibition on eight viral outbreaks.
The COVID-19 pandemic in the Democratic Republic of the Congo was a part of the worldwide pandemic of coronavirus disease 2019 caused by severe acute respiratory syndrome coronavirus 2. The virus was confirmed to have reached the Democratic Republic of the Congo on 10 March 2020. The first few confirmed cases were all outside arrivals.

The COVID-19 pandemic in Benin was a part of the ongoing worldwide pandemic of coronavirus disease 2019 caused by severe acute respiratory syndrome coronavirus 2. The virus was confirmed to have reached Benin in March 2020.
Fractional dose vaccination is a strategy to reduce the dose of a vaccine to achieve a vaccination policy goal that is more difficult to achieve with conventional vaccination approaches, including deploying a vaccine faster in a pandemic, reaching more individuals in the setting of limited healthcare budgets, or minimizing side effects due to the vaccine.



