Medicare is an unofficial designation used to refer to the publicly funded single-payer healthcare system of Canada. Canada's health care system consists of 13 provincial and territorial health insurance plans, which provide universal healthcare coverage to Canadian citizens, permanent residents, and depending on the province or territory, certain temporary residents. The systems are individually administered on a provincial or territorial basis, within guidelines set by the federal government. The formal terminology for the insurance system is provided by the Canada Health Act and the health insurance legislation of the individual provinces and territories.

An emergency department (ED), also known as an accident and emergency department (A&E), emergency room (ER), emergency ward (EW) or casualty department, is a medical treatment facility specializing in emergency medicine, the acute care of patients who present without prior appointment; either by their own means or by that of an ambulance. The emergency department is usually found in a hospital or other primary care center.

A clinic is a health facility that is primarily focused on the care of outpatients. Clinics can be privately operated or publicly managed and funded. They typically cover the primary care needs of populations in local communities, in contrast to larger hospitals which offer more specialized treatments and admit inpatients for overnight stays.
Health care in Ireland is delivered through public and private healthcare. The public health care system is governed by the Health Act 2004, which established a new body to be responsible for providing health and personal social services to everyone living in Ireland – the Health Service Executive. The new national health service came into being officially on 1 January 2005; however the new structures are currently in the process of being established as the reform programme continues. In addition to the public-sector, there is also a large private healthcare market.

The health care system in Japan provides different types of services, including screening examinations, prenatal care and infectious disease control, with the patient accepting responsibility for 30% of these costs while the government pays the remaining 70%. Payment for personal medical services is offered by a universal health care insurance system that provides relative equality of access, with fees set by a government committee. All residents of Japan are required by the law to have health insurance coverage. People without insurance from employers can participate in a national health insurance program, administered by local governments. Patients are free to select physicians or facilities of their choice and cannot be denied coverage. Hospitals, by law, must be run as non-profits and be managed by physicians.
A public hospital, or government hospital, is a hospital which is government owned and is fully funded by the government and operates solely off the money that is collected from taxpayers to fund healthcare initiatives. In some countries, this type of hospital provides medical care free of charge to patients, covering expenses and wages by government reimbursement.

Health care in Saudi Arabia is a national health care system in which the government provides free universal healthcare coverage through a number of government agencies. There is also a growing role and increased participation from the private sector in the provision of health care services. Saudi Arabia has been ranked among the 26 best countries in providing high quality healthcare.

The National Healthcare Group (NHG) is a group of healthcare institutions in Singapore. The group was formed in 2000 and operates several hospitals, national specialty centers, and polyclinics. Tan Tock Seng Hospital is the largest hospital in the group and serves as the flagship hospital for the cluster.

Healthcare in the United Kingdom is a devolved matter, with England, Northern Ireland, Scotland and Wales each having their own systems of publicly funded healthcare, funded by and accountable to separate governments and parliaments, together with smaller private sector and voluntary provision. As a result of each country having different policies and priorities, a variety of differences have developed between these systems since devolution.

The Swedish health care system is mainly government-funded, universal for all citizens and decentralized, although private health care also exists. The health care system in Sweden is financed primarily through taxes levied by county councils and municipalities. A total of 21 councils are in charge with primary and hospital care within the country.
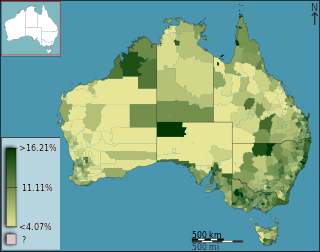
Health care in Australia operates under a shared public-private model underpinned by the Medicare system, the national single-payer funding model. State and territory governments operate public health facilities where eligible patients receive care free of charge. Primary health services, such as GP clinics, are privately owned in most situations, but attract Medicare rebates. Australian citizens, permanent residents, and some visitors and visa holders are eligible for health services under the Medicare system. Individuals are encouraged through tax surcharges to purchase health insurance to cover services offered in the private sector, and further fund health care.
Healthcare in England is mainly provided by the National Health Service (NHS), a public body that provides healthcare to all permanent residents in England, that is free at the point of use. The body is one of four forming the UK National Health Service as health is a devolved matter; there are differences with the provisions for healthcare elsewhere in the United Kingdom, and in England it is overseen by NHS England. Though the public system dominates healthcare provision in England, private health care and a wide variety of alternative and complementary treatments are available for those willing and able to pay.
Healthcare in Algeria consists of an established network of hospitals, clinics, and dispensaries. The government provides universal health care.

Healthcare in Israel is universal and participation in a medical insurance plan is compulsory. All Israeli residents are entitled to basic health care as a fundamental right. The Israeli healthcare system is based on the National Health Insurance Law of 1995, which mandates all citizens resident in the country to join one of four official health insurance organizations, known as Kupat Holim which are run as not-for-profit organizations and are prohibited by law from denying any Israeli resident membership. Israelis can increase their medical coverage and improve their options by purchasing private health insurance. In a survey of 48 countries in 2013, Israel's health system was ranked fourth in the world in terms of efficiency, and in 2014 it ranked seventh out of 51. In 2020, Israel's health system was ranked third most efficient in the world. In 2015, Israel was ranked sixth-healthiest country in the world by Bloomberg rankings and ranked eighth in terms of life expectancy.

Healthcare in Singapore is under the purview of the Ministry of Health of the Government of Singapore. It mainly consists of a government-run publicly funded universal healthcare system as well as a significant private healthcare sector. Financing of healthcare costs is done through a mixture of direct government subsidies, compulsory comprehensive savings, national healthcare insurance, and cost-sharing.

A hospital is a healthcare institution providing patient treatment with specialized health science and auxiliary healthcare staff and medical equipment. The best-known type of hospital is the general hospital, which typically has an emergency department to treat urgent health problems ranging from fire and accident victims to a sudden illness. A district hospital typically is the major health care facility in its region, with many beds for intensive care and additional beds for patients who need long-term care. Specialized hospitals include trauma centers, rehabilitation hospitals, children's hospitals, seniors' (geriatric) hospitals, and hospitals for dealing with specific medical needs such as psychiatric treatment and certain disease categories. Specialized hospitals can help reduce health care costs compared to general hospitals. Hospitals are classified as general, specialty, or government depending on the sources of income received.

The healthcare system of New Zealand has undergone significant changes throughout the past several decades. From an essentially fully public system based on the Social Security Act 1938, reforms have introduced market and health insurance elements primarily since the 1980s, creating a mixed public-private system for delivering healthcare.
In South Africa, private and public health systems exist in parallel. The public system serves the vast majority of the population. Authority and service delivery are divided between the national Department of Health, provincial health departments, and municipal health departments.

Italy's healthcare system is consistently ranked among the best in the world. Life expectancy is the 4th highest among OECD countries and the world's 8th highest according to the WHO. Healthcare spending accounted for 9.7% of GDP in 2020.
Examples of health care systems of the world, sorted by continent, are as follows.