The term abdominal surgery broadly covers surgical procedures that involve opening the abdomen (laparotomy). Surgery of each abdominal organ is dealt with separately in connection with the description of that organ Diseases affecting the abdominal cavity are dealt with generally under their own names.

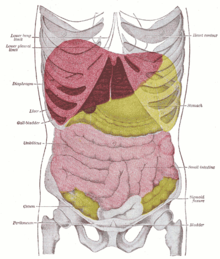
The abdominal cavity is a large body cavity in humans and many other animals that contains many organs. It is a part of the abdominopelvic cavity. It is located below the thoracic cavity, and above the pelvic cavity. Its dome-shaped roof is the thoracic diaphragm, a thin sheet of muscle under the lungs, and its floor is the pelvic inlet, opening into the pelvis.

Peritonitis is inflammation of the localized or generalized peritoneum, the lining of the inner wall of the abdomen and cover of the abdominal organs. Symptoms may include severe pain, swelling of the abdomen, fever, or weight loss. One part or the entire abdomen may be tender. Complications may include shock and acute respiratory distress syndrome.
A laparotomy is a surgical procedure involving a surgical incision through the abdominal wall to gain access into the abdominal cavity. It is also known as a celiotomy.

An injury is any physiological damage to living tissue caused by immediate physical stress. An injury can occur intentionally or unintentionally and may be caused by blunt trauma, penetrating trauma, burning, toxic exposure, asphyxiation, or overexertion. Injuries can occur in any part of the body, and different symptoms are associated with different injuries.
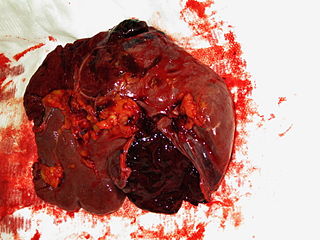
A splenic injury, which includes a ruptured spleen, is any injury to the spleen. The rupture of a normal spleen can be caused by trauma, such as a traffic collision.

Pneumoperitoneum is pneumatosis in the peritoneal cavity, a potential space within the abdominal cavity. The most common cause is a perforated abdominal organ, generally from a perforated peptic ulcer, although any part of the bowel may perforate from a benign ulcer, tumor or abdominal trauma. A perforated appendix seldom causes a pneumoperitoneum.

Blunt trauma, also known as blunt force trauma or non-penetrating trauma, is physical traumas, and particularly in the elderly who fall. It is contrasted with penetrating trauma which occurs when an object pierces the skin and enters a tissue of the body, creating an open wound and bruise.
Hemoperitoneum is the presence of blood in the peritoneal cavity. The blood accumulates in the space between the inner lining of the abdominal wall and the internal abdominal organs. Hemoperitoneum is generally classified as a surgical emergency; in most cases, urgent laparotomy is needed to identify and control the source of the bleeding. In selected cases, careful observation may be permissible. The abdominal cavity is highly distensible and may easily hold greater than five liters of blood, or more than the entire circulating blood volume for an average-sized individual. Therefore, large-scale or rapid blood loss into the abdomen will reliably induce hemorrhagic shock and, if untreated, may rapidly lead to death.
Blunt splenic trauma occurs when a significant impact to the spleen from some outside source damages or ruptures the spleen. Treatment varies depending on severity, but often consists of embolism or splenectomy.
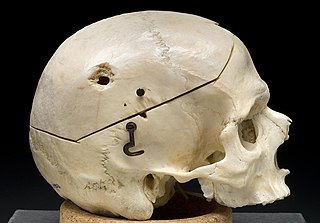
A gunshot wound (GSW) is a penetrating injury caused by a projectile from a gun. Damages may include bleeding, bone fractures, organ damage, wound infection, loss of the ability to move part of the body and, in more severe cases, death. Damage depends on the part of the body hit, the path the bullet follows through the body, and the type and speed of the bullet. Long-term complications can include lead poisoning and post-traumatic stress disorder (PTSD).

Penetrating trauma is an open wound injury that occurs when an object pierces the skin and enters a tissue of the body, creating a deep but relatively narrow entry wound. In contrast, a blunt or non-penetrating trauma may have some deep damage, but the overlying skin is not necessarily broken and the wound is still closed to the outside environment. The penetrating object may remain in the tissues, come back out the path it entered, or pass through the full thickness of the tissues and exit from another area.
Abdominal guarding is the tensing of the abdominal wall muscles to guard inflamed organs within the abdomen from the pain of pressure upon them. The tensing is detected when the abdominal wall is pressed. Abdominal guarding is also known as 'défense musculaire'.

The abdominopelvic cavity is a body cavity that consists of the abdominal cavity and the pelvic cavity. The upper portion is the abdominal cavity, and it contains the stomach, liver, pancreas, spleen, gallbladder, kidneys, small intestine, and most of the large intestine. The lower portion is the pelvic cavity, and it contains the urinary bladder, the rest of the large intestine, and the internal reproductive organs.

Diaphragmatic rupture is a tear of the diaphragm, the muscle across the bottom of the ribcage that plays a crucial role in breathing. Most commonly, acquired diaphragmatic tears result from physical trauma. Diaphragmatic rupture can result from blunt or penetrating trauma and occurs in about 0.5% of all people with trauma.
An exploratory laparotomy is a general surgical operation where the abdomen is opened and the abdominal organs are examined for injury or disease. It is the standard of care in various blunt and penetrating trauma situations in which there may be life-threatening internal injuries. It is also used in certain diagnostic situations, in which the operation is undertaken in search of a unifying cause for multiple signs and symptoms of disease, and in the staging of some cancers.

A stab wound is a specific form of penetrating trauma to the skin that results from a knife or a similar pointed object. While stab wounds are typically known to be caused by knives, they can also occur from a variety of implements, including broken bottles and ice picks. Most stabbings occur because of intentional violence or through self-infliction. The treatment is dependent on many different variables such as the anatomical location and the severity of the injury. Even though stab wounds are inflicted at a much greater rate than gunshot wounds, they account for less than 10% of all penetrating trauma deaths.

A liver injury, also known as liver laceration, is some form of trauma sustained to the liver. This can occur through either a blunt force such as a car accident, or a penetrating foreign object such as a knife. Liver injuries constitute 5% of all traumas, making it the most common abdominal injury. Generally nonoperative management and observation is all that is required for a full recovery.
A pancreatic injury is some form of trauma sustained by the pancreas. The injury can be sustained through either blunt forces, such as a motor vehicle accident, or penetrative forces, such as that of a gunshot wound. The pancreas is one of the least commonly injured organs in abdominal trauma.
Splenosis is the result of spleen tissue breaking off the main organ and implanting at another site inside the body. This is called heterotopic autotransplantation of the spleen. It most commonly occurs as a result of traumatic splenic rupture or abdominal surgery. Depending on the location of the spleen, the new piece usually implants in another part of the abdominal cavity. Single case reports also describe splenosis in the thoracic cavity, in subcutaneous tissue, in the liver or in the cranial cavity. Splenosis must be distinguished from the presence of additional spleens, which are innate and are the result of differences in embryological development. Additionally, splenosis must be differentiated from malignant tumors which may look similar when imaged.