
Interstitial cystitis (IC), a type of bladder pain syndrome (BPS), is chronic pain in the bladder and pelvic floor of unknown cause. It is the urologic chronic pelvic pain syndrome of women. Symptoms include feeling the need to urinate right away, needing to urinate often, and pain with sex. IC/BPS is associated with depression and lower quality of life. Many of those affected also have irritable bowel syndrome and fibromyalgia.
A urinary tract infection (UTI) is an infection that affects part of the urinary tract. When it affects the lower urinary tract it is known as a bladder infection (cystitis) and when it affects the upper urinary tract it is known as a kidney infection (pyelonephritis). Symptoms from a lower urinary tract infection include pain with urination, frequent urination, and feeling the need to urinate despite having an empty bladder. Symptoms of a kidney infection include fever and flank pain usually in addition to the symptoms of a lower UTI. Rarely the urine may appear bloody. In the very old and the very young, symptoms may be vague or non-specific.

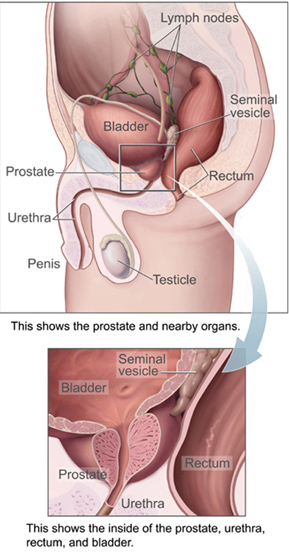
Prostatitis is an umbrella term for a variety of medical conditions that incorporate bacterial and non-bacterial origin illnesses in the pelvic region. In contrast with the plain meaning of the word, the diagnosis may not always include inflammation. Prostatitis is classified into acute, chronic, asymptomatic inflammatory prostatitis, and chronic pelvic pain syndrome.

Prostate massage is the massage or stimulation of the male prostate gland for medical purposes or sexual stimulation.

Levofloxacin, sold under the brand name Levaquin among others, is an antibiotic medication. It is used to treat a number of bacterial infections including acute bacterial sinusitis, pneumonia, H. pylori, urinary tract infections, chronic prostatitis, and some types of gastroenteritis. Along with other antibiotics it may be used to treat tuberculosis, meningitis, or pelvic inflammatory disease. Use is generally recommended only when other options are not available. It is available by mouth, intravenously, and in eye drop form.
Glomerulation refers to bladder hemorrhages which are thought to be associated with some types of interstitial cystitis (IC).

Urinary retention is an inability to completely empty the bladder. Onset can be sudden or gradual. When of sudden onset, symptoms include an inability to urinate and lower abdominal pain. When of gradual onset, symptoms may include loss of bladder control, mild lower abdominal pain, and a weak urine stream. Those with long-term problems are at risk of urinary tract infections.

Ofloxacin is a quinolone antibiotic useful for the treatment of a number of bacterial infections. When taken by mouth or injection into a vein, these include pneumonia, cellulitis, urinary tract infections, prostatitis, plague, and certain types of infectious diarrhea. Other uses, along with other medications, include treating multidrug resistant tuberculosis. An eye drop may be used for a superficial bacterial infection of the eye and an ear drop may be used for otitis media when a hole in the ear drum is present.

Mycoplasmataceae is a family of bacteria in the order Mycoplasmatales. This family consists of the genera Mycoplasma and Ureaplasma.

Pyelonephritis is inflammation of the kidney, typically due to a bacterial infection. Symptoms most often include fever and flank tenderness. Other symptoms may include nausea, burning with urination, and frequent urination. Complications may include pus around the kidney, sepsis, or kidney failure.
Urethral syndrome is defined as symptoms suggestive of a lower urinary tract infection but in the absence of significant bacteriuria with a conventional pathogen. It is a diagnosis of exclusion in patients with dysuria and frequency without demonstrable infection. In women, vaginitis should also be ruled out.

Norfloxacin, sold under the brand name Noroxin among others, is an antibiotic that belongs to the class of fluoroquinolone antibiotics. It is used to treat urinary tract infections, gynecological infections, inflammation of the prostate gland, gonorrhea and bladder infection. Eye drops were approved for use in children older than one year of age.
Prostatic congestion is a medical condition of the prostate gland that happens when the prostate becomes swollen by excess fluid and can be caused by prostatosis. The condition often results in a person with prostatic congestion feeling the urge to urinate frequently. Prostatic congestion has been associated with prostate disease, which can progress due to age. Oftentimes, the prostate will grow in size which can lead to further problems, such as prostatitis, enlarged prostate, or prostate cancer.
Acute prostatitis is a serious bacterial infection of the prostate gland. This infection is a medical emergency. It should be distinguished from other forms of prostatitis such as chronic bacterial prostatitis and chronic pelvic pain syndrome (CPPS).
Lower urinary tract symptoms (LUTS) refer to a group of clinical symptoms involving the bladder, urinary sphincter, urethra and, in men, the prostate. The term is more commonly applied to men—over 40% of older men are affected—but lower urinary tract symptoms also affect women. The condition is also termed prostatism in men, but LUTS is preferred.

Chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS), previously known as chronic nonbacterial prostatitis, is long-term pelvic pain and lower urinary tract symptoms (LUTS) without evidence of a bacterial infection. It affects about 2–6% of men. Together with IC/BPS, it makes up urologic chronic pelvic pain syndrome (UCPPS).
Asymptomatic inflammatory prostatitis is a painless inflammation of the prostate gland where there is no evidence of infection. It should be distinguished from the other categories of prostatitis characterised by either pelvic pain or evidence of infection, such as chronic bacterial prostatitis, acute bacterial prostatitis and chronic pelvic pain syndrome (CPPS). It is a common finding in men with benign prostatic hyperplasia.
Urologic diseases or conditions include urinary tract infections, kidney stones, bladder control problems, and prostate problems, among others. Some urologic conditions do not affect a person for that long and some are lifetime conditions. Kidney diseases are normally investigated and treated by nephrologists, while the specialty of urology deals with problems in the other organs. Gynecologists may deal with problems of incontinence in women.

Quinolone antibiotics constitute a large group of broad-spectrum bacteriocidals that share a bicyclic core structure related to the substance 4-quinolone. They are used in human and veterinary medicine to treat bacterial infections, as well as in animal husbandry, specifically poultry production.
Urologic chronic pelvic pain syndrome (UCPPS) is ongoing bladder pain in either sex, chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS) in men and interstitial cystitis or painful bladder syndrome (IC/PBS) in women.



