Related Research Articles
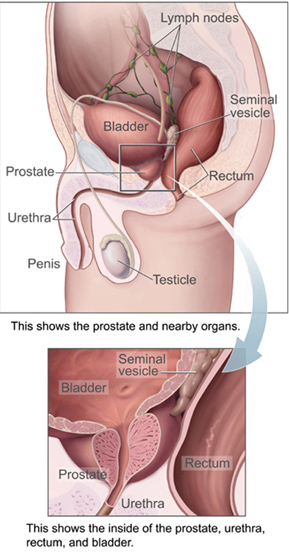
The prostate is both an accessory gland of the male reproductive system and a muscle-driven mechanical switch between urination and ejaculation. It is found in all male mammals. It differs between species anatomically, chemically, and physiologically. Anatomically, the prostate is found below the bladder, with the urethra passing through it. It is described in gross anatomy as consisting of lobes and in microanatomy by zone. It is surrounded by an elastic, fibromuscular capsule and contains glandular tissue, as well as connective tissue.

Retrograde ejaculation occurs when semen which would be ejaculated via the urethra is redirected to the urinary bladder. Normally, the sphincter of the bladder contracts before ejaculation, sealing the bladder which besides inhibiting the release of urine also prevents a reflux of seminal fluids into the male bladder during ejaculation. The semen is forced to exit via the urethra, the path of least resistance. When the bladder sphincter does not function properly, retrograde ejaculation may occur. It can also be induced deliberately by a male as a primitive form of male birth control or as part of certain alternative medicine practices. The retrograde-ejaculated semen, which goes into the bladder, is excreted with the next urination.

The seminal vesicles are a pair of convoluted tubular glands that lie behind the urinary bladder of some male mammals. They secrete fluid that partly composes the semen.
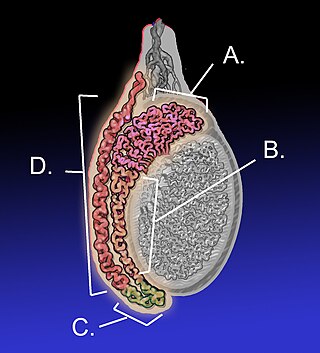
The epididymis is an elongated tubular structure attached to the posterior side of each one of the two male reproductive glands, the testes. It is a single, narrow, tightly coiled tube in adult humans, 6 to 7 meters in length. It connects the testicle to the vas deferens in the male reproductive system. The epididymis serves as an interconnection between the multiple efferent ducts at the rear of a testicle (proximally), and the vas deferens (distally). Its primary function is the storage, maturation and transport of sperm cells.

The vas deferens, with the more modern name ductus deferens, is part of the male reproductive system of many vertebrates. The ducts transport sperm from the epididymis to the ejaculatory ducts in anticipation of ejaculation. The vas deferens is a partially coiled tube which exits the abdominal cavity through the inguinal canal.

The ejaculatory ducts are paired structures in male reproductive system. Each ejaculatory duct is formed by the union of the vas deferens with the duct of the seminal vesicle. They pass through the prostate, and open into the urethra above the seminal colliculus. During ejaculation, semen passes through the prostate gland, enters the urethra and exits the body via the urinary meatus.
The male reproductive system consists of a number of sex organs that play a role in the process of human reproduction. These organs are located on the outside of the body and within the pelvis.

The human reproductive system includes the male reproductive system which functions to produce and deposit sperm; and the female reproductive system which functions to produce egg cells, and to protect and nourish the fetus until birth. Humans have a high level of sexual differentiation. In addition to differences in nearly every reproductive organ, there are numerous differences in typical secondary sex characteristics.

Azoospermia is the medical condition of a man whose semen contains no sperm. It is associated with male infertility, but many forms are amenable to medical treatment. In humans, azoospermia affects about 1% of the male population and may be seen in up to 20% of male infertility situations in Canada.
Terms oligospermia, oligozoospermia, and low sperm count refer to semen with a low concentration of sperm and is a common finding in male infertility. Often semen with a decreased sperm concentration may also show significant abnormalities in sperm morphology and motility. There has been interest in replacing the descriptive terms used in semen analysis with more quantitative information.
Aspermia is the complete lack of semen with ejaculation. It is associated with infertility.
Male infertility refers to a sexually mature male's inability to impregnate a fertile female. In humans it accounts for 40–50% of infertility. It affects approximately 7% of all men. Male infertility is commonly due to deficiencies in the semen, and semen quality is used as a surrogate measure of male fecundity. More recently, advance sperm analyses that examine intracellular sperm components are being developed.
Anejaculation is the pathological inability to ejaculate despite an erection in males, with (orgasmic) or without (anorgasmic) orgasm.

Reproductive medicine is a branch of medicine concerning the male and female reproductive systems. It encompasses a variety of reproductive conditions, their prevention and assessment, as well as their subsequent treatment and prognosis.

A semen analysis, also called seminogram or spermiogram, evaluates certain characteristics of a male's semen and the sperm contained therein. It is done to help evaluate male fertility, whether for those seeking pregnancy or verifying the success of vasectomy. Depending on the measurement method, just a few characteristics may be evaluated or many characteristics may be evaluated. Collection techniques and precise measurement method may influence results.
Semen quality is a measure of male fertility, a measure of the ability of sperm in semen to accomplish fertilization. Semen quality involves both sperm quantity and quality. Semen quality is a major factor for fertility.

In human anatomy, the penis is an external male intromittent organ that additionally serves as the urinary duct. The main parts are the root (radix); the body (corpus); and the epithelium of the penis including the shaft skin and the foreskin (prepuce) covering the glans penis. The body of the penis is made up of three columns of tissue: two corpora cavernosa on the dorsal side and corpus spongiosum between them on the ventral side. The human male urethra passes through the prostate gland, where it is joined by the ejaculatory duct, and then through the penis. The urethra traverses the corpus spongiosum, and its opening, the meatus, lies on the tip of the glans penis. It is a passage both for urination and ejaculation of semen.

Semen, also known as seminal fluid, is an organic bodily fluid created to contain spermatozoa. It is secreted by the gonads and other sexual organs of male or hermaphroditic animals and can fertilize the female ovum. Semen is produced and originates from the seminal vesicle, which is located in the pelvis. The process that results in the discharge of semen from the urethral orifice is called ejaculation. In humans, seminal fluid contains several components besides spermatozoa: proteolytic and other enzymes as well as fructose are elements of seminal fluid which promote the survival of spermatozoa, and provide a medium through which they can move or "swim". The fluid is adapted to be discharged deep into the vagina, so the spermatozoa can pass into the uterus and form a zygote with an egg.

Ejaculation is the discharge of semen from the male reproductive tract as a result of an orgasm. It is the final stage and natural objective of male sexual stimulation, and an essential component of natural conception. Ejaculation can occur spontaneously during sleep, and is a normal part of human sexual development. In rare cases, ejaculation occurs because of prostatic disease. Anejaculation is the condition of being unable to ejaculate. Ejaculation is usually very pleasurable for men; dysejaculation is an ejaculation that is painful or uncomfortable. Retrograde ejaculation is the condition where semen travels backwards into the bladder rather than out of the urethra.
Ejaculatory duct obstruction (EDO) is a pathological condition which is characterized by the obstruction of one or both ejaculatory ducts. Thus, the efflux of semen is not possible. It can be congenital or acquired. It is a cause of male infertility and/or pelvic pain. Ejaculatory duct obstruction must not be confused with an obstruction of the vas deferens.
References
- 1 2 3 4 5 Shaw, Wilfred (2015). Shaw's textbook of gynaecology. Wilfred Shaw, V. Padubidri, Shirish Daftary, John Howkins, Gordon Bourne (16th ed.). New Delhi. ISBN 978-81-312-3872-1. OCLC 904687532.
{{cite book}}: CS1 maint: location missing publisher (link) - 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 Robin G, Marcelli F, Mitchell V, Marchetti C, Lemaitre L, Dewailly D, Leroy-Billiard M, Rigot JM (2008). "[Why and how to assess hypospermia?]". Gynecol Obstet Fertil. 36 (10): 1035–42. doi:10.1016/j.gyobfe.2008.04.021. PMID 18801689.
- ↑ Bassas Arnau, Lluís (2009). "[Exploration of testicular function]". Endocrinologia y Nutricion. 56 (1): 18–31. doi:10.1016/S1575-0922(09)70190-1. ISSN 1575-0922. PMID 19627705.
- ↑ Semet, M.; Paci, M.; Saïas-Magnan, J.; Metzler-Guillemain, C.; Boissier, R.; Lejeune, H.; Perrin, J. (2017). "The impact of drugs on male fertility: a review". Andrology. 5 (4): 640–663. doi: 10.1111/andr.12366 . PMID 28622464.
- 1 2 3 4 Salas-Huetos, Albert; James, Emma R.; Aston, Kenneth I.; Jenkins, Timothy G.; Carrell, Douglas T. (2019). "Diet and sperm quality: Nutrients, foods and dietary patterns". Reproductive Biology. 19 (3): 219–224. doi:10.1016/j.repbio.2019.07.005. ISSN 2300-732X. PMID 31375368. S2CID 199387538.
- ↑ La Vignera, Sandro; Vita, Roberto (2018). "Thyroid dysfunction and semen quality". International Journal of Immunopathology and Pharmacology. 32: 2058738418775241. doi:10.1177/2058738418775241. ISSN 2058-7384. PMC 5946587 . PMID 29737216.
- ↑ Ricci, Elena; Al Beitawi, Suha; Cipriani, Sonia; Candiani, Massimo; Chiaffarino, Francesca; Viganò, Paola; Noli, Stefania; Parazzini, Fabio (2017). "Semen quality and alcohol intake: a systematic review and meta-analysis". Reproductive Biomedicine Online. 34 (1): 38–47. doi: 10.1016/j.rbmo.2016.09.012 . ISSN 1472-6491. PMID 28029592.
- ↑ Guo, Dan; Xu, Min; Zhou, Qifan; Wu, Chunhua; Ju, Rong; Dai, Jiazhen (2019). "Is low body mass index a risk factor for semen quality? A PRISMA-compliant meta-analysis". Medicine. 98 (32): e16677. doi:10.1097/MD.0000000000016677. ISSN 1536-5964. PMC 6709190 . PMID 31393367.
- ↑ Salas-Huetos, Albert; Maghsoumi-Norouzabad, Leila; James, Emma R.; Carrell, Douglas T.; Aston, Kenneth I.; Jenkins, Timothy G.; Becerra-Tomás, Nerea; Javid, Ahmad Zare; Abed, Reza; Torres, Pedro Javier; Luque, Eugenia Mercedes (2021). "Male adiposity, sperm parameters and reproductive hormones: An updated systematic review and collaborative meta-analysis". Obesity Reviews. 22 (1): e13082. doi:10.1111/obr.13082. ISSN 1467-789X. PMID 32705766. S2CID 220730623.
- 1 2 Zhao, Jiang; Dong, Xingyou; Hu, Xiaoyan; Long, Zhou; Wang, Liang; Liu, Qian; Sun, Bishao; Wang, Qingqing; Wu, Qingjian; Li, Longkun (2016). "Zinc levels in seminal plasma and their correlation with male infertility: A systematic review and meta-analysis". Scientific Reports. 6: 22386. Bibcode:2016NatSR...622386Z. doi:10.1038/srep22386. ISSN 2045-2322. PMC 4773819 . PMID 26932683.
- ↑ Salas-Huetos, Albert; Bulló, Mònica; Salas-Salvadó, Jordi (2017). "Dietary patterns, foods and nutrients in male fertility parameters and fecundability: a systematic review of observational studies". Human Reproduction Update. 23 (4): 371–389. doi: 10.1093/humupd/dmx006 . ISSN 1460-2369. PMID 28333357.
- ↑ Ricci, Elena; Viganò, Paola; Cipriani, Sonia; Somigliana, Edgardo; Chiaffarino, Francesca; Bulfoni, Alessandro; Parazzini, Fabio (2017). "Coffee and caffeine intake and male infertility: a systematic review". Nutrition Journal. 16 (1): 37. doi: 10.1186/s12937-017-0257-2 . ISSN 1475-2891. PMC 5482951 . PMID 28646871.
- ↑ Sunder, Meera; Leslie, Stephen W. (2021), "Semen Analysis", StatPearls, Treasure Island (FL): StatPearls Publishing, PMID 33232039 , retrieved 2021-07-30
- ↑ Gonzales, Gustavo F.; Gonzales, Carla; Gonzales-Castañeda, Cynthia (2009). "Lepidium meyenii (Maca): a plant from the highlands of Peru--from tradition to science". Forschende Komplementärmedizin. 16 (6): 373–380. doi:10.1159/000264618. ISSN 1661-4127. PMID 20090350. S2CID 9721063.
- ↑ Rigot, J.-M.; Marcelli, F.; Giuliano, F. (2013). "Troubles de l'éjaculation à l'exception de l'éjaculation prématurée, troubles de l'orgasme". Progrès en Urologie (in French). 23 (9): 657–663. doi:10.1016/j.purol.2013.01.011. PMID 23830260.
- ↑ Althof, Stanley E. (2016). "Psychosexual therapy for premature ejaculation". Translational Andrology and Urology. 5 (4): 475–481. doi: 10.21037/tau.2016.05.15 . ISSN 2223-4691. PMC 5001981 . PMID 27652220.
- ↑ Hanson, Brent M.; Aston, Kenneth I.; Jenkins, Tim G.; Carrell, Douglas T.; Hotaling, James M. (2018). "The impact of ejaculatory abstinence on semen analysis parameters: a systematic review". Journal of Assisted Reproduction and Genetics. 35 (2): 213–220. doi:10.1007/s10815-017-1086-0. ISSN 1573-7330. PMC 5845044 . PMID 29143943.
- ↑ Roberts, Matthew; Jarvi, Keith (2009). "Steps in the investigation and management of low semen volume in the infertile man". Canadian Urological Association Journal. 3 (6): 479–485. doi:10.5489/cuaj.1180. ISSN 1911-6470. PMC 2792416 . PMID 20019978.
- ↑ Jurewicz, Michael; Gilbert, Bruce R. (2016). "Imaging and angiography in male factor infertility". Fertility and Sterility. 105 (6): 1432–1442. doi: 10.1016/j.fertnstert.2016.04.009 . ISSN 1556-5653. PMID 27125229.
- ↑ Coppens, L. (1997). "[Diagnosis and treatment of obstructive seminal vesicle pathology]". Acta Urologica Belgica. 65 (2): 11–19. ISSN 0001-7183. PMID 9324904.
- 1 2 Pan, Michael M.; Hockenberry, Mark S.; Kirby, Edgar W.; Lipshultz, Larry I. (2018). "Male Infertility Diagnosis and Treatment in the Era of In Vitro Fertilization and Intracytoplasmic Sperm Injection". Medical Clinics of North America. 102 (2): 337–347. doi:10.1016/j.mcna.2017.10.008. PMID 29406062.
- ↑ Cissen, Maartje; Bensdorp, Alexandra; Cohlen, Ben J; Repping, Sjoerd; de Bruin, Jan Peter; van Wely, Madelon (2016). Cochrane Gynaecology and Fertility Group (ed.). "Assisted reproductive technologies for male subfertility". Cochrane Database of Systematic Reviews. 2016 (2): CD000360. doi:10.1002/14651858.CD000360.pub5. PMC 10335364 . PMID 26915339.
- ↑ Weinberg, May; Sar-Shalom Nahshon, Chen; Feferkorn, Ido; Bornstein, Jacob (2020). "Evaluation of human papilloma virus in semen as a risk factor for low sperm quality and poor in vitro fertilization outcomes: a systematic review and meta-analysis". Fertility and Sterility. 113 (5): 955–969.e4. doi: 10.1016/j.fertnstert.2020.01.010 . PMID 32386620. S2CID 218585082.
- ↑ "HPV Vaccine Recommendations | CDC". www.cdc.gov. 2021. Retrieved 2021-08-04.
{{cite web}}: CS1 maint: url-status (link)