Hookworm infection is an infection by a type of intestinal parasite known as a hookworm.[1][5] Initially, itching and a rash may occur at the site of infection. Those only affected by a few worms may show no symptoms. Those infected by many worms may experience abdominal pain, diarrhea, weight loss, and tiredness. The mental and physical development of children may be affected. Anemia may result.[1]
Two common hookworm infections in humans are ancylostomiasis and necatoriasis, caused by the species Ancylostoma duodenale and Necator americanus respectively. Hookworm eggs are deposited in the stools of infected people. If these end up in the environment, they can hatch into larvae (immature worms), which can then penetrate the skin. One type can also be spread through contaminated food. Risk factors include walking barefoot in warm climates, where sanitation is poor. Diagnosis is by examination of a stool sample with a microscope.[1]
The disease can be prevented on an individual level by not walking barefoot in areas where the disease is common. At a population level, decreasing outdoor defecation, not using raw feces as fertilizer, and mass deworming are effective.[1] Treatment is typically with the medications albendazole or mebendazole for one to three days. Iron supplements may be needed in those with anemia.[3]
Hookworms infected about 428 million people in 2015.[4] Heavy infections can occur in both children and adults, but are less common in adults.[2] They are rarely fatal.[6] Hookworm infection is a soil-transmitted helminthiasis and classified as a neglected tropical disease.[7]
Signs and symptoms
No symptoms or signs are specific for hookworm infection, but they give rise to a combination of intestinal inflammation and progressive iron-deficiency anemia and protein deficiency. Coughing, chest pain, wheezing, and fever sometimes result from severe infection. Epigastric pains, indigestion, nausea, vomiting, constipation, and diarrhea can occur early or in later stages, as well, although gastrointestinal symptoms tend to improve with time. Signs of advanced severe infection are those of anemia and protein deficiency, including emaciation, cardiac failure, and abdominal distension with ascites.[citation needed]
Larval invasion of the skin (mostly in the Americas) can produce a skin disease called cutaneous larva migrans also known as creeping eruption. The hosts of these worms are not human and the larvae can only penetrate the upper five layers of the skin, where they give rise to intense, local itching, usually on the foot or lower leg, known as ground itch. This infection is due to larvae from the A. braziliense hookworm. The larvae migrate in tortuous tunnels between the stratum basale and stratum corneum of the skin, causing serpiginous vesicular lesions. With advancing movement of the larvae, the rear portions of the lesions become dry and crusty. The lesions are typically intensely itchy.[8]
Incubation period
The incubation period can vary between a few weeks to many months, and is largely dependent on the number of hookworm parasites an individual is infected with.[9]
A. duodenale worms are grayish white or pinkish with the head slightly bent in relation to the rest of the body. This bend forms a definitive hook shape at the anterior end for which hookworms are named. They possess well-developed mouths with two pairs of teeth. While males measure approximately one centimeter by 0.5 millimeter, the females are often longer and stouter. Additionally, males can be distinguished from females based on the presence of a prominent posterior copulatory bursa.[11]
N. americanus is very similar in morphology to A. duodenale. N. americanus is generally smaller than A. duodenale with males usually 5 to 9mm long and females about 1cm long. Whereas A. duodenale possesses two pairs of teeth, N. americanus possesses a pair of cutting plates in the buccal capsule. Additionally, the hook shape is much more defined in Necator than in Ancylostoma.[11]
The hookworm thrives in warm soil where temperatures are over 18°C (64°F). They exist primarily in sandy or loamy soil and cannot live in clay or muck. Rainfall averages must be more than 1,000mm (39in) a year for them to survive. Only if these conditions exist can the eggs hatch. Infective larvae of N. americanus can survive at higher temperatures, whereas those of A. duodenale are better adapted to cooler climates. Generally, they live for only a few weeks at most under natural conditions, and die almost immediately on exposure to direct sunlight or desiccation.[citation needed]
Infection of the host is by the larvae, not the eggs. While A. duodenale can be ingested, the usual method of infection is through the skin; this is commonly caused by walking barefoot through areas contaminated with fecal matter. The larvae are able to penetrate the skin of the foot, and once inside the body, they migrate through the vascular system to the lungs, and from there up the trachea, and are swallowed. They then pass down the esophagus and enter the digestive system, finishing their journey in the intestine, where the larvae mature into adult worms.[12][13]
Once in the host gut, Necator tends to cause a prolonged infection, generally 1 to 5 years (many worms die within a year or two of infecting), though some adult worms have been recorded to live for 15 years or more. Ancylostoma adults are short-lived, surviving on average for only about 6 months. However, the infection can be prolonged because dormant larvae can be "recruited" sequentially from tissue "stores" (see Pathology, above) over many years, to replace expired adult worms. This can give rise to seasonal fluctuations in infection prevalence and intensity (apart from normal seasonal variations in transmission).[citation needed]
They mate inside the host, females laying from 10,000 to 30,000 eggs per day and some 15 to 56 million eggs during their adult lifetimes, which pass out in feces. Because 5 to 7 weeks are needed for adult worms to mature, mate, and produce eggs, in the early stages of very heavy infection, acute symptoms might occur without any eggs being detected in the patient's feces. This can make diagnosis very difficult.[citation needed]
N. americanus and A. duodenale eggs can be found in warm, moist soil where they eventually hatch into first-stage larvae, or L1. L1, the feeding noninfective rhabditoform stage, will feed on soil microbes and eventually molt into second-stage larvae, L2, which is also in the rhabditoform stage. It will feed for about 7 days and then molt into the third-stage larvae, or L3. This is the filariform stage of the parasite, that is, the nonfeeding infective form of the larvae. The L3 larvae are extremely motile and seek higher ground to increase their chances of penetrating the skin of a human host. The L3 larvae can survive up to 2 weeks without finding a host. While N. americanus larvae only infect through penetration of skin, A. duodenale can infect both through penetration and orally. After the L3 larvae have successfully entered the host, they then travel through the subcutaneous venules and lymphatic vessels of the human host. Eventually, the L3 larvae enter the lungs through the pulmonary capillaries and break out into the alveoli. They then travel up the trachea to be coughed and swallowed by the host. After being swallowed, the L3 larvae are then found in the small intestine, where they molt into the L4, or adult worm stage. The entire process from skin penetration to adult development takes about 5–9 weeks. The female adult worms release eggs (N. americanus about 9,000–10,000 eggs/day and A. duodenale 25,000–30,000 eggs/day), which are passed in the feces of the human host. These eggs hatch in the environment within several days and the cycle starts anew.[12][14][15]
Pathophysiology
Hookworm infection is generally considered to be asymptomatic, but as Norman Stoll described in 1962, it is an extremely dangerous infection because its damage is "silent and insidious."[16] An individual may experience general symptoms soon after infection. Ground-itch, which is an allergic reaction at the site of parasitic penetration and entry, is common in patients infected with N. americanus.[11] Additionally, cough and pneumonitis may result as the larvae begin to break into the alveoli and travel up the trachea. Then once the larvae reach the small intestine of the host and begin to mature, the infected individual will experience diarrhea and other gastrointestinal discomfort.[11] However, the "silent and insidious" symptoms referred to by Stoll are related to chronic, heavy-intensity hookworm infections. Major morbidity associated with hookworm infection is caused by intestinal blood loss, iron deficiency anemia, and protein malnutrition.[14] They result mainly from adult hookworms in the small intestine ingesting blood, rupturing erythrocytes, and degrading hemoglobin in the host.[12] This long-term blood loss can manifest itself physically through facial and peripheral edema; eosinophilia and pica/geophagy caused by iron deficiency anemia are also experienced by some hookworm-infected patients.[11] Recently, more attention has been given to other important outcomes of hookworm infection that play a large role in public health. It is now widely accepted that children who have chronic hookworm infection can experience growth retardation as well as intellectual and cognitive impairments.[12][17] Additionally, recent research has focused on the potential of adverse maternal-fetal outcomes when the mother is infected with hookworm during pregnancy.[citation needed]
The disease was linked to nematode worms (Ankylostoma duodenalis) from one-third to half an inch long in the intestine chiefly through the labours of Theodor Bilharz and Griesinger in Egypt (1854).[18]
The symptoms can be linked to inflammation in the gut stimulated by feeding hookworms, such as nausea, abdominal pain and intermittent diarrhea, and to progressive anemia in prolonged disease: capricious appetite, pica/geophagy (or dirt-eating), obstinate constipation followed by diarrhea, palpitations, thready pulse, coldness of the skin, pallor of the mucous membranes, fatigue and weakness, shortness of breath and in cases running a fatal course, dysentery, hemorrhages and edema.[18] The worms suck blood and damage the mucosa. However, the blood loss in the stools is not visibly apparent.[citation needed]
Blood tests in early infection often show a rise in numbers of eosinophils, a type of white blood cell that is preferentially stimulated by worm infections in tissues (large numbers of eosinophils are also present in the local inflammatory response). Falling blood hemoglobin levels will be seen in cases of prolonged infection with anemia.[citation needed]
In contrast to most intestinal helminthiases, where the heaviest parasitic loads tend to occur in children, hookworm prevalence and intensity can be higher among adult males. The explanation for this is that hookworm infection tends to be occupational, so that coworkers and other close groups maintain a high prevalence of infection among themselves by contaminating their work environment. However, in most endemic areas, adult women are the most severely affected by anemia, mainly because they have much higher physiological needs for iron (menstruation, repeated pregnancy).An interesting consequence of this in the case of Ancylostoma duodenale infection is translactational transmission of infection: the skin-invasive larvae of this species do not all immediately pass through the lungs and on into the gut, but spread around the body via the circulation, to become dormant inside muscle fibers. In a pregnant woman, after childbirth some or all of these larvae are stimulated to re-enter the circulation (presumably by sudden hormonal changes), then to pass into the mammary glands, so that the newborn baby can receive a large dose of infective larvae through its mother's milk. This accounts for otherwise inexplicable cases of very heavy, even fatal, hookworm infections in children a month or so of age, in places such as China, India and northern Australia. An identical phenomenon is much more commonly seen with Ancylostoma caninum infections in dogs, where the newborn pups can even die of hemorrhaging from their intestines caused by massive numbers of feeding hookworms. This also reflects the close evolutionary link between the human and canine parasites, which probably have a common ancestor dating back to when humans and dogs first started living closely together. Filariform larvae is the infective stage of the parasite: infection occurs when larvae in soil penetrate the skin, or when they are ingested through contaminated food and water following skin penetration.[citation needed]
Diagnosis
Hookworm egg
Diagnosis depends on finding characteristic worm eggs on microscopic examination of the stools, although this is not possible in early infection. Early signs of infection in most dogs include limbular limping and anal itching. The eggs are oval or elliptical, measuring 60 by 40µm, colorless, not bile stained and with a thin transparent hyaline shell membrane. When released by the worm in the intestine, the egg contains an unsegmented ovum. During its passage down the intestine, the ovum develops and thus the eggs passed in feces have a segmented ovum, usually with 4 to 8 blastomeres. As the eggs of both Ancylostoma and Necator (and most other hookworm species) are indistinguishable, to identify the genus, they must be cultured in the lab to allow larvae to hatch out. If the fecal sample is left for a day or more under tropical conditions, the larvae will have hatched out, so eggs might no longer be evident. In such a case, it is essential to distinguish hookworms from Strongyloides larvae, as infection with the latter has more serious implications and requires different management. The larvae of the two hookworm species can also be distinguished microscopically, although this would not be done routinely, but usually for research purposes. Adult worms are rarely seen (except via endoscopy, surgery or autopsy), but if found, would allow definitive identification of the species. Classification can be performed based on the length of the buccal cavity, the space between the oral opening and the esophagus: hookworm rhabditoform larvae have long buccal cavities whereas Strongyloides rhabditoform larvae have short buccal cavities.[11]
Recent research has focused on the development of DNA-based tools for diagnosis of infection, specific identification of hookworm, and analysis of genetic variability within hookworm populations.[19] Because hookworm eggs are often indistinguishable from other parasitic eggs, PCR assays could serve as a molecular approach for accurate diagnosis of hookworm in the feces.[19][20]
The infective larvae develop and survive in an environment of damp dirt, particularly sandy and loamy soil. They cannot survive in clay or muck. The main lines of precaution are those dictated by good hygiene behaviors:
Deworm pet dogs and cats. Canine and feline hookworms rarely develop to adulthood in humans. Ancylostoma caninum, the common dog hookworm, occasionally develops into an adult to cause eosinophilic enteritis in people, but their invasive larvae can cause an itchy rash called cutaneous larva migrans.
Moxidectin is available in the United States as (imidacloprid + moxidectin) topical solution for dogs and cats. It utilizes moxidectin for control and prevention of roundworms, hookworms, heartworms, and whipworms.
Ethiopian children treated for schistosoma and hookworms
Children
Most of these public health concerns have focused on children who are infected with hookworm. This focus on children is largely due to the large body of evidence that has demonstrated strong associations between hookworm infection and impaired learning, increased absences from school, and decreased future economic productivity.[12] In 2001, the 54th World Health Assembly passed a resolution demanding member states to attain a minimum target of regular deworming of at least 75% of all at-risk school children by the year 2010.[21] A 2008 World Health Organization publication reported on these efforts to treat at-risk school children. Some of the interesting statistics were as follows: 1) only 9 out of 130 endemic countries were able to reach the 75% target goal; and 2) less than 77 million school-aged children (of the total 878 million at risk) were reached, which means that only 8.78% of at-risk children are being treated for hookworm infection.[22]
School-based mass deworming
School-based mass deworming programs have been the most popular strategy to address the issue of hookworm infection in children. School-based programs are extremely cost-effective as schools already have an available, extensive, and sustained infrastructure with a skilled workforce that has a close relationship with the community.[21] With little training from a local health system, teachers can easily administer the drugs which often cost less than US$0.50 per child per year.[23]
Recently, many people have begun to question if the school-based programs are necessarily the most effective approach. An important concern with school-based programs is that they often do not reach children who do not attend school, thus ignoring a large number of at-risk children. A 2008 study by Massa et al. continued the debate regarding school-based programs. They examined the effects of community-directed treatments versus school-based treatments in the Tanga Region of Tanzania. A major conclusion was that the mean infection intensity of hookworm was significantly lower in the villages employing the community-directed treatment approach than the school-based approach. The community-directed treatment model used in this specific study allowed villagers to take control of the child's treatment by having villagers select their own community drug distributors to administer the antihelminthic drugs. Additionally, villagers organized and implemented their own methods for distributing the drugs to all children.[24] The positive results associated with this new model highlight the need for large-scale community involvement in deworming campaigns.[citation needed]
Public health education
Many mass deworming programs also combine their efforts with a public health education. These health education programs often stress important preventative techniques such as: washing your hands before eating, and staying away from water/areas contaminated by human feces. These programs may also stress that shoes must be worn, however, these come with their own health risks and may not be effective.[25] Shoe wearing patterns in towns and villages across the globe are determined by cultural beliefs, and the levels of education within that society. The wearing of shoes will prevent the entry of hookworm infections from the surrounding soils into tender skin regions; such as areas between the toes.[26]
Sanitation
Historical examples, such as the hookworm campaigns in Mississippi and Florida from 1943 to 1947 have shown that the primary cause of hookworm infection is poor sanitation, which can be solved by building and maintaining toilets. But while these may seem like simple tasks, they raise important public health challenges. Most infected populations are from poverty-stricken areas with very poor sanitation. Thus, it is most likely that at-risk children do not have access to clean water to wash their hands and live in environments with no proper sanitation infrastructure. Health education, therefore, must address preventive measures in ways that are both feasible and sustainable in the context of resource-limited settings.[citation needed]
Integrated approaches
Evaluation of numerous public health interventions has generally shown that improvement in each individual component ordinarily attributed to poverty (for example, sanitation, health education and underlying nutrition status) often have minimal impact on transmission. For example, one study found that the introduction of latrines into a resource-limited community only reduced the prevalence of hookworm infection by four percent.[27] However, another study in Salvador, Brazil found that improved drainage and sewerage had a significant impact on the prevalence of hookworm infection but no impact at all on the intensity of hookworm infection.[28] This seems to suggest that environmental control alone has a limited but incomplete effect on the transmission of hookworms. It is imperative, therefore, that more research is performed to understand the efficacy and sustainability of integrated programs that combine numerous preventive methods including education, sanitation, and treatment.
The most common treatment for hookworm are benzimidazoles, specifically albendazole and mebendazole. BZAs kill adult worms by binding to the nematode's β-tubulin and subsequently inhibiting microtubule polymerization within the parasite.[14] In certain circumstances, levamisole and pyrantel pamoate may be used.[12] A 2008 review found that the efficacy of single-dose treatments for hookworm infections were as follows: 72% for albendazole, 15% for mebendazole, and 31% for pyrantel pamoate.[29] This substantiates prior claims that albendazole is much more effective than mebendazole for hookworm infections. Also of note is that the World Health Organization does recommend anthelmintic treatment in pregnant women after the first trimester.[14] It is also recommended that if the patient also has anemia that ferrous sulfate (200mg) be administered three times daily at the same time as anthelmintic treatment; this should be continued until hemoglobin values return to normal which could take up to 3 months.[11]
Hookworm infection can be treated with local cryotherapy when the hookworm is still in the skin.[30]
Albendazole is effective both in the intestinal stage and during the stage the parasite is still migrating under the skin.[30]
In case of anemia, iron supplementation can cause relief symptoms of iron-deficiency anemia. However, as red blood cell levels are restored, shortage of other essentials such as folic acid or vitamin B12 may develop, so these might also be supplemented.
During the 1910s, common treatments for hookworm included thymol, 2-naphthol, chloroform, gasoline, and eucalyptus oil.[31] By the 1940s, the treatment of choice used tetrachloroethylene,[32] given as 3 to 4 cc in the fasting state, followed by 30 to 45 g of sodium sulfate. Tetrachloroethylene was reported to have a cure rate of 80 percent for Necator infections, but 25 percent in Ancylostoma infections, and often produced mild intoxication in the patient.
Reinfection and drug resistance
Other important issues related to the treatment of hookworm are reinfection and drug resistance. It has been shown that reinfection after treatment can be extremely high. Some studies even show that 80% of pretreatment hookworm infection rates can be seen in treated communities within 30–36 months.[14] While reinfection may occur, it is still recommended that regular treatments be conducted as it will minimize the occurrence of chronic outcomes. There are also increasing concerns about the issue of drug resistance. Drug resistance has appeared in front-line anthelmintics used for livestock nematodes. Generally human nematodes are less likely to develop resistance due to longer reproducing times, less frequent treatment, and more targeted treatment. Nonetheless, the global community must be careful to maintain the effectiveness of current anthelmintic as no new anthelmintic drugs are in the late-stage development.[14]
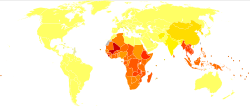
It is estimated that between 576 and 740 million individuals are infected with hookworm.[33][14] Of these infected individuals, about 80 million are severely affected.[19] The major cause of hookworm infection is N. americanus which is found in the Americas, sub-Saharan Africa, and Asia.[12]A. duodenale is found in more scattered focal environments, namely Europe and the Mediterranean. Most infected individuals are concentrated in sub-Saharan Africa and East Asia/the Pacific Islands with each region having estimates of 198 million and 149 million infected individuals, respectively. Other affected regions include: South Asia (50 million), Latin America and the Caribbean (50 million), South Asia (59 million), Middle East/North Africa (10 million).[14] A majority of these infected individuals live in poverty-stricken areas with poor sanitation. Hookworm infection is most concentrated among the world's poorest who live on less than $2 a day.[12]
While hookworm infection may not directly lead to mortality, its effects on morbidity demand immediate attention. When considering disability-adjusted life years (DALYs), neglected tropical diseases, including hookworm infection, rank among diarrheal diseases, ischemic heart disease, malaria, and tuberculosis as one of the most important health problems of the developing world.
It has been estimated that as many as 22.1 million DALYs have been lost due to hookworm infection. Recently, there has been increasing interest to address the public health concerns associated with hookworm infection. For example, the Bill & Melinda Gates Foundation recently donated US$34 million to fight Neglected Tropical Diseases including hookworm infection.[34] Former US President Clinton also announced a mega-commitment at the Clinton Global Initiative (CGI) 2008 Annual Meeting to de-worm 10 million children.[35]
Many of the numbers regarding the prevalence of hookworm infection are estimates as there is no international surveillance mechanism currently in place to determine prevalence and global distribution.[12] Some prevalence rates have been measured through survey data in endemic regions around the world. The following are some of the most recent findings on prevalence rates in regions endemic with hookworm.
There have also been technological developments that may facilitate more accurate mapping of hookworm prevalence. Some researchers have begun to use geographical information systems (GIS) and remote sensing (RS) to examine helminth ecology and epidemiology. Brooker et al. utilized this technology to create helminth distribution maps of sub-Saharan Africa. By relating satellite derived environmental data with prevalence data from school-based surveys, they were able to create detailed prevalence maps. The study focused on a wide range of helminths, but interesting conclusions about hookworm specifically were found. As compared to other helminths, hookworm is able to survive in much hotter conditions and was highly prevalent throughout the upper end of the thermal range.[43]
Improved molecular diagnostic tools are another technological advancement that could help improve existing prevalence statistics. Recent research has focused on the development of a DNA-based tool that can be used for diagnosis of infection, specific identification of hookworm, and analysis of genetic variability in hookworm populations. Again this can serve as a major tool for different public health measures against hookworm infection. Most research regarding diagnostic tools is now focused on the creation of a rapid and cost-effective assay for the specific diagnosis of hookworm infection. Many are hopeful that its development can be achieved within the next five years.[when?][19]
History
Discovery
The symptoms now attributed to hookworm appear in papyrus papers of ancient Egypt (c.1500 BC), described as a derangement characterized by anemia. Avicenna, a Persian physician of the eleventh century, discovered the worm in several of his patients and related it to their disease. In later times, the condition was noticeably prevalent in the mining industry in England, France, Germany, Belgium, North Queensland, and elsewhere.[18]
Italian physician Angelo Dubini was the modern-day discoverer of the worm in 1838 after an autopsy of a peasant woman. Dubini published details in 1843 and identified the species as A. duodenale. Working in the Egyptian medical system in 1852 German physician Theodor Bilharz, drawing upon the work of colleague Wilhelm Griesinger, found these worms during autopsies and went a step further in linking them to local endemic occurrences of chlorosis, which would probably be called iron-deficiency anemia today.
A breakthrough came 25 years later following a diarrhea and anemia epidemic that took place among Italian workmen employed on the Gotthard Rail Tunnel.[18] In an 1880 paper, physicians Camillo Bozzolo, Edoardo Perroncito, and Luigi Pagliani correctly hypothesized that hookworm was linked to the fact that workers had to defecate inside the 15km tunnel, and that many wore worn-out shoes.[44] The work environment often contained standing water, sometimes knee-deep, and the larvae were capable of surviving several weeks in the water, allowing them to infect many of the workers. In 1897, it was established that the skin was the principal avenue of infection and the biological life cycle of the hookworm was clarified.
Eradication programmes
In 1899, American zoologist Charles Wardell Stiles identified progressive pernicious anemia seen in the southern United States as being caused by the hookworm A. duodenale. Testing in the 1900s revealed very heavy infestations in school-age children. In Puerto Rico, Dr. Bailey K. Ashford, a US Army physician, organized and conducted a parasite treatment campaign, which cured approximately 300,000 people (one-third of the Puerto Rican population) and reduced the death rate from this anemia by 90 percent during the years 1903–04.
On October 26, 1909, the Rockefeller Sanitary Commission for the Eradication of Hookworm Disease was organized as a result of a gift of US$1 million from John D. Rockefeller, Sr. The five-year program was a remarkable success and a great contribution to the United States' public health, instilling public education, medication, field work and modern government health departments in eleven southern states.[45] The hookworm exhibit was a prominent part of the 1910 Mississippi state fair.
The commission found that an average of 40% of school-aged children were infected with hookworm. Areas with higher levels of hookworm infection prior to the eradication program experienced greater increases in school enrollment, attendance, and literacy after the intervention. Econometric studies have shown that this effect cannot be explained by a variety of alternative factors, including differential trends across areas, changing crop prices, shifts in certain educational and health policies and the effect of malaria eradication.[46] No significant contemporaneous results were found for adults who should have benefited less from the intervention owing to their substantially lower (prior) infection rates. The program nearly eradicated hookworm and would flourish afterward with new funding as the Rockefeller FoundationInternational Health Division.[47]
The RF's hookworm campaign in Mexico showed how science and politics play a role in developing health policies. It brought together government officials, health officials, public health workers, Rockefeller officials and the community. This campaign was launched to eradicate hookworms in Mexico. Although the campaign did not focus on long-term treatments, it did set the terms of the relationship between Mexico and the Rockefeller Foundation. The scientific knowledge behind this campaign helped shape public health policies, improved public health and built a strong relationship between US and Mexico.[48]
In the 1920s, hookworm eradication reached the Caribbean and Latin America, where great mortality was reported among people in the West Indies towards the end of the 18th century, as well as through descriptions sent from Brazil and various other tropical and sub-tropical regions.[18]
Treatments
Treatment in the early 20th century relied on the use of Epsom salt to reduce protective mucus, followed by thymol to kill the worms.[49][31] By the 1940s, tetrachloroethylene was the leading method.[32] It was not until later in the mid-20th century when new organic drug compounds were developed.[50]
Research
Anemia in pregnancy
It is estimated that a third of all pregnant women in developing countries are infected with hookworm, 56% of all pregnant women in developing countries experience anemia, 20% of all maternal deaths are either directly or indirectly related to anemia. Numbers like this have led to an increased interest in the topic of hookworm-related anemia during pregnancy.[51] With the understanding that chronic hookworm infection can often lead to anemia, many people are now questioning if the treatment of hookworm could effect change in severe anemia rates and thus also on maternal and child health as well. Most evidence suggests that the contribution of hookworm to maternal anemia merits that all women of child-bearing age living in endemic areas be subject to periodic anthelmintic treatment. The World Health Organization even recommends that infected pregnant women be treated after their first trimester.[14] Regardless of these suggestions, only Madagascar, Nepal and Sri Lanka have added deworming to their antenatal care programs.[52]
This lack of deworming of pregnant women is explained by the fact that most individuals still fear that anthelmintic treatment will result in adverse birth outcomes. But a 2006 study by Gyorkos et al. found that when comparing a group of pregnant women treated with mebendazole with a control placebo group, both illustrated rather similar rates in adverse birth outcomes. The treated group demonstrated 5.6% adverse birth outcomes, while the control group had 6.25% adverse birth outcomes.[51] Furthermore, Larocque et al. illustrated that treatment for hookworm infection actually led to positive health results in the infant. This study concluded that treatment with mebendazole plus iron supplements during antenatal care significantly reduced the proportion of very low birth weight infants when compared to a placebo control group.[53] Studies so far have validated recommendations to treat infected pregnant women for hookworm infection during pregnancy.
A review found that a single dose of antihelminthics (anti-worm drugs) given in the second trimester of pregnancy "may reduce maternal anaemia and worm prevalence when used in settings with high prevalence of maternal helminthiasis".[54]
The intensity of hookworm infection as well as the species of hookworm have yet to be studied as they relate to hookworm-related anemia during pregnancy. Additionally, more research must be done in different regions of the world to see if trends noted in completed studies persist.[citation needed]
Malaria co-infection
Co-infection with hookworm and Plasmodium falciparum is common in Africa.[55] Although exact numbers are unknown, preliminary analyses estimate that as many as a quarter of African schoolchildren (17.8–32.1 million children aged 5–14 years) may be coincidentally at-risk of both P. falciparum and hookworm.[56] While original hypotheses stated that co-infection with multiple parasites would impair the host's immune response to a single parasite and increase susceptibility to clinical disease, studies have yielded contrasting results. For example, one study in Senegal showed that the risk of clinical malaria infection was increased in helminth-infected children in comparison to helminth-free children while other studies have failed to reproduce such results,[57] and even among laboratory mouse experiments the effect of helminths on malaria is variable.[58]
Some hypotheses and studies suggest that helminth infections may protect against cerebral malaria due to the possible modulation of pro-inflammatory and anti-inflammatory cytokines responses.[59] Furthermore, the mechanisms underlying this supposed increased susceptibility to disease are unknown. For example, helminth infections cause potent and highly polarized immune response characterized by increased T-helper cell type 2 (Th2) cytokine and Immunoglobulin E (IgE) production.[60] However, the effect of such responses on the human immune response is unknown. Additionally, both malaria and helminth infection can cause anemia, but the effect of co-infection and possible enhancement of anemia is poorly understood.[50]
The hygiene hypothesis states that infants and children who lack exposure to infectious agents are more susceptible to allergic diseases via modulation of immune system development. The theory was first proposed by David P. Strachan who noted that hay fever and eczema were less common in children who belonged to large families.[61] Since then, studies have noted the effect of gastrointestinal worms on the development of allergies in the developing world. For example, a study in Gambia found that eradication of worms in some villages led to increased skin reactions to allergies among children.[62]
While annual or semi-annual mass antihelminthic administration is a critical aspect of any public health intervention, many have begun to realize how unsustainable it is due to aspects such as poverty, high rates of re-infection, and diminished efficacy of drugs with repeated use. Current research, therefore, has focused on the development of a vaccine that could be integrated into existing control programs. The goal of vaccine development is not necessarily to create a vaccine with sterilizing immunity or complete protection against immunity. A vaccine that reduces the likelihood of vaccinated individuals developing severe infections and thus reduced blood and nutrient levels could still have a significant impact on the high burden of disease throughout the world.
Current research focuses on targeting two stages in the development of the worm: the larval stage and the adult stage. Research on larval antigens has focused on proteins that are members of the pathogenesis-related protein superfamily, Ancylostoma Secreted Proteins.[63] Although they were first described in Anyclostoma, these proteins have also been successfully isolated from the secreted product of N. americanus. N. americanus ASP-2 (Na-ASP-2) is currently the leading larval-stage hookworm vaccine candidate. A randomized, double-blind, placebo-controlled study has already been performed; 36 healthy adults without a history of hookworm infection were given three intramuscular injections of three different concentrations of Na-ASP-2 and observed for six months after the final vaccination.[64] The vaccine induced significant anti-Na-ASP-2 IgG and cellular immune responses. In addition, it was safe and produced no debilitating side effects. The vaccine is now in a phase one trial; healthy adult volunteers with documented evidence of previous infection in Brazil are being given the same dose concentration on the same schedule used in the initial study.[63] If this study is successful, the next step would be to conduct a phase two trial to assess the rate and intensity of hookworm infection among vaccinated persons. Because the Na-ASP-2 vaccine only targets the larval stage, it is critical that all subjects enrolled in the study be treated with antihelminthic drugs to eliminate adult worms prior to vaccination.
Adult hookworm antigens have also been identified as potential candidates for vaccines. When adult worms attach to the intestinal mucosa of the human host, erythrocytes are ruptured in the worm's digestive tract which causes the release of free hemoglobin which is subsequently degraded by a proteolytic cascade. Several of these proteins that are responsible for this proteolytic cascade are also essential for the worm's nutrition and survival.[65] Therefore, a vaccine that could induce antibodies for these antigens could interfere with the hookworm's digestive pathway and impair the worm's survival. Three proteins have been identified: the aspartic protease-hemoglobinase APR-1, the cysteine protease-hemoglobinase CP-2, and a glutathione S-transferase.[66][67][68] Vaccination with APR-1 and CP-2 led to reduced host blood loss and fecal egg counts in dogs.[66][67] With APR-1, vaccination even led to reduced worm burden.[66] Research is currently stymied at the development of at least one of these antigens as a recombinant protein for testing in clinical trials.
Terminology
The term "hookworm" is sometimes used to refer to hookworm infection.[12] A hookworm is a type of parasitic worm (helminth).
Trichuriasis, also known as whipworm infection, is an infection by the parasitic worm Trichuris trichiura (whipworm). If infection is only with a few worms, there are often no symptoms. In those who are infected with many worms, there may be abdominal pain, fatigue and diarrhea. The diarrhea sometimes contains blood. Infections in children may cause poor intellectual and physical development. Low red blood cell levels may occur due to loss of blood.
Helminthiasis, also known as worm infection, is any macroparasitic disease of humans and other animals in which a part of the body is infected with parasitic worms, known as helminths. There are numerous species of these parasites, which are broadly classified into tapeworms, flukes, and roundworms. They often live in the gastrointestinal tract of their hosts, but they may also burrow into other organs, where they induce physiological damage.
Necator americanus is a species of hookworm commonly known as the New World hookworm. Like other hookworms, it is a member of the phylum Nematoda. It is an obligatory parasitic nematode that lives in the small intestine of human hosts. Necatoriasis—a type of helminthiasis—is the term for the condition of being host to an infestation of a species of Necator. Since N. americanus and Ancylostoma duodenale are the two species of hookworms that most commonly infest humans, they are usually dealt with under the collective heading of "hookworm infection". They differ most obviously in geographical distribution, structure of mouthparts, and relative size.
Parasitic worms, also known as helminths, are large macroparasites; adults can generally be seen with the naked eye. Many are intestinal worms that are soil-transmitted and infect the gastrointestinal tract. Other parasitic worms such as schistosomes reside in blood vessels.
Ancylostoma duodenale is a species of the roundworm genus Ancylostoma. It is a parasitic nematode worm and commonly known as the Old World hookworm. It lives in the small intestine of hosts such as humans, cats and dogs, where it is able to mate and mature. Ancylostoma duodenale and Necator americanus are the two human hookworm species that are normally discussed together as the cause of hookworm infection. They are dioecious. Ancylostoma duodenale is abundant throughout the world, including Southern Europe, North Africa, India, China, southeast Asia, some areas in the United States, the Caribbean, and South America.
Uncinaria stenocephala is a nematode that parasitizes dogs, cats, and foxes as well as humans. It is rare to find in cats in the United States. Uncinaria stenocephala is the most common canine hookworm in cooler regions, such as Canada and the northern regions of the US, where it can be found primarily in foxes (40%). U. stenocephala is also one of the most common hookworms in the UK, called the northern hookworm, however it has a rather low prevalence. U. stenocephala is also considered to be zoonotic hookworms because they live in animals but can be transmitted to humans.
The soil-transmitted helminths are a group of intestinal parasites belonging to the phylum Nematoda that are transmitted primarily through contaminated soil. They are so called because they have a direct life cycle which requires no intermediate hosts or vectors, and the parasitic infection occurs through faecal contamination of soil, foodstuffs and water supplies. The adult forms are essentially parasites of humans, causing soil-transmitted helminthiasis (STH), but also infect domesticated mammals. The juveniles are the infective forms and they undergo tissue-migratory stages during which they invade vital organs such as lungs and liver. Thus the disease manifestations can be both local and systemic. The geohelminths together present an enormous infection burden on humanity, amounting to 135,000 deaths every year, and persistent infection of more than two billion people.
Ancylostomiasis is a hookworm disease caused by infection with Ancylostoma hookworms. The name is derived from Greek ancylos αγκύλος "crooked, bent" and stoma στόμα "mouth".
Necatoriasis is the condition of infection by Necator hookworms, such as Necator americanus. This hookworm infection is a type of helminthiasis (infection) which is a type of neglected tropical disease.
Deworming is the giving of an anthelmintic drug to a human or animals to rid them of helminths parasites, such as roundworm, flukes and tapeworm. Purge dewormers for use in livestock can be formulated as a feed supplement that is eaten, a paste or gel that is deposited at the back of the animal's mouth, a liquid drench given orally, an injectable, or as a pour-on which can be applied to the animal's topline. In dogs and cats, purge dewormers come in many forms including a granular form to be added to food, pill form, chew tablets, and liquid suspensions.
Oesophagostomum is a genus of parasitic nematodes (roundworms) of the family Strongylidae. These worms occur in Africa, Brazil, China, Indonesia and the Philippines. The majority of human infection with Oesophagostomum is localized to northern Togo and Ghana. Because the eggs may be indistinguishable from those of the hookworms, the species causing human helminthomas are rarely identified with accuracy. Oesophagostomum, especially O. bifurcum, are common parasites of livestock and animals like goats, pigs and non-human primates, although it seems that humans are increasingly becoming favorable hosts as well. The disease they cause, oesophagostomiasis, is known for the nodule formation it causes in the intestines of its infected hosts, which can lead to more serious problems such as dysentery. Although the routes of human infection have yet to be elucidated sufficiently, it is believed that transmission occurs through oral-fecal means, with infected humans unknowingly ingesting soil containing the infectious filariform larvae.
Hookworm vaccine is a vaccine against hookworm. No effective vaccine for the disease in humans has yet been developed. Hookworms, parasitic nematodes transmitted in soil, infect approximately 700 million humans, particularly in tropical regions of the world where endemic hookworms include Ancylostoma duodenale and Necator americanus. Hookworms feed on blood and those infected with hookworms may develop chronic anaemia and malnutrition. Helminth infection can be effectively treated with benzimidazole drugs, and efforts led by the World Health Organization have focused on one to three yearly de-worming doses in schools because hookworm infections with the heaviest intensities are most common in school-age children. However, these drugs only eliminate existing adult parasites and re-infection can occur soon after treatment. School-based de-worming efforts do not treat adults or pre-school children and concerns exist about drug resistance developing in hookworms against the commonly used treatments, thus a vaccine against hookworm disease is sought to provide more permanent resistance to infection.
Ancylostoma braziliense is a species of hookworm belonging to the genus Ancylostoma. It is an intestinal parasite of domestic cats and dogs. Severe infection is often fatal to these pets, especially in puppies and kittens. The infection is particularly endemic in the southern United States. It is most often confused with the zoonotic hookworm species Ancylostoma ceylanicum because of their uncanny resemblance.
Ancylostoma caninum is a species of nematode known as a hookworm, which principally infects the small intestine of dogs. The result of A. caninum infection ranges from asymptomatic cases to death of the dog; better nourishment, increasing age, prior A. caninum exposure, or vaccination are all linked to improved survival. Other hosts include carnivores such as wolves, foxes, and cats, with a small number of cases having been reported in humans.
The Ancylostomatidae are a family of worms that includes the hookworms.
Anthelmintics or antihelminthics are a group of antiparasitic drugs that expel parasitic worms (helminths) and other internal parasites from the body by either stunning or killing them and without causing significant damage to the host. They may also be called vermifuges or vermicides. Anthelmintics are used to treat people who are infected by helminths, a condition called helminthiasis. These drugs are also used to treat infected animals.
Soil-transmitted helminthiasis is a type of worm infection (helminthiasis) caused by different species of roundworms. It is caused specifically by those worms which are transmitted through soil contaminated with faecal matter and are therefore called soil-transmitted helminths. Three types of soil-transmitted helminthiasis can be distinguished: ascariasis, hookworm infection and whipworm infection. These three types of infection are therefore caused by the large roundworm A. lumbricoides, the hookworms Necator americanus or Ancylostoma duodenale and by the whipworm Trichuris trichiura.
Children Without Worms (CWW) is a program of the Task Force for Global Health and envisions a world in which all at-risk people, specifically targeting children, are healthy and free of worm infections (helminthiases) so they can develop to their full potential. To accomplish the vision of a worm-free world, CWW works closely with the World Health Organization, national Ministries of Health, nongovernmental organizations and private-public coalitions such as Uniting to Combat NTDs. It acts as an intermediary for the pharmaceutical company Johnson and Johnson in distributing the latter's mebendazole for mass deworming of children to reduce or end soil-transmitted helminthiasis.
Ancylostoma ceylanicum is a parasitic roundworm belonging to the genus Ancylostoma. It is a hookworm both of humans and of other mammals such as dogs, cats, and golden hamsters. It is the only zoonotic hookworm species that is able to produce symptomatic infections in humans, with the majority of cases being in Southeast Asia.
Hookworms are intestinal, blood-feeding, parasitic roundworms that cause types of infection known as helminthiases. Hookworm infection is found in many parts of the world, and is common in areas with poor access to adequate water, sanitation, and hygiene. In humans, infections are caused by two main species of roundworm, belonging to the genera Ancylostoma and Necator. In other animals the main parasites are species of Ancylostoma. Hookworm is closely associated with poverty because it is most often found in impoverished areas, and its symptoms promote poverty through the educational and health effects it has on children. It is the leading cause of anemia and undernutrition in developing countries, while being one of the most commonly occurring diseases among poor people. Hookworm thrives in areas where rainfall is sufficient and keeps the soil from drying out, and where temperatures are higher, making rural, coastal areas prime conditions for the parasite to breed.
↑ Prevention, CDC - Centers for Disease Control and. "CDC - Hookworm - Biology". www.cdc.gov. Archived from the original on 21 June 2017. Retrieved 21 June 2017.
1 2 3 4 5 6 7 Markell, Edward K.; John, David C.; Petri, William H. (2006). Markell and Voge's medical parasitology (9thed.). St. Louis, Mo: Elsevier Saunders. ISBN978-0-7216-4793-7.
↑ Massa K, Magnussen P, Sheshe A, Ntakamulenga R, Ndawi B, Olsen A (2009). "The effect of the community-directed treatment approach versus the school-based treatment approach on the prevalence and intensity of schistosomiasis and soil-transmitted helminthiasis among schoolchildren in Tanzania". Trans. R. Soc. Trop. Med. Hyg. 103 (1): 31–37. doi:10.1016/j.trstmh.2008.07.009. PMID18771789.
↑ Howell, Daniel (2010). The Barefoot Book: 50 Great Reasons to Kick Off Your Shoes. Hunter House. ISBN978-0897935548.
↑ Huttly SR (1990). "The impact of inadequate sanitary conditions on health in developing countries". World Health Stat. Q. 43 (3): 118–26. PMID2146815.
1 2 Albanese G, Venturi C, Galbiati G (2001). "Treatment of larva migrans cutanea (creeping eruption): A comparison between albendazole and traditional therapy". Int. J. Dermatol. 40 (1): 67–71. doi:10.1046/j.1365-4362.2001.01103.x. PMID11277961. S2CID40314184.
↑ "Global network for neglected tropical diseases receives $34 million from Gates Foundation: IDB leads campaign to greatly reduce the burden of most neglected diseases by 2020 in Latin America and the Caribbean." Press Release. Global Network for Neglected Tropical Diseases. 30 January 2009.
↑ "Deworm the World at Clinton Global Initiative 2008 Annual Meeting: up to 10 million children to benefit from deworming!" Press Release. Deworm the World, 2008.
↑ Pal D, Chattopadhyay UK, Sengupta G (April 2007). "A study on the prevalence of hookworm infection in four districts of West Bengal and its linkage with anemia". Indian J. Pathol. Microbiol. 50 (2): 449–52. PMID17883107.
↑ Gandhi NS, Jizhang C, Khoshnood K, Fuying X, Shanwen L, Yaoruo L, Bin Z, Haechou X, Chongjin T, Yan W, Wensen W, Dungxing H, Chong C, Shuhua X, Hawdon JM, Hotez PJ (August 2001). "Epidemiology of Necator americanus hookworm infections in Xiulongkan Village, Hainan Province, China: high prevalence and intensity among middle-aged and elderly residents". J. Parasitol. 87 (4): 739–43. doi:10.1645/0022-3395(2001)087[0739:EONAHI]2.0.CO;2. PMID11534635. S2CID28630527.
↑ Fleming FM, Brooker S, Geiger SM, Caldas IR, Correa-Oliveira R, Hotez PJ, Bethony JM (January 2006). "Synergistic associations between hookworm and other helminth species in a rural community in Brazil". Trop. Med. Int. Health. 11 (1): 56–64. doi:10.1111/j.1365-3156.2005.01541.x. PMID16398756. S2CID20407618.
↑ Brooker S, Clements AC, Bundy DA (2006). "Global epidemiology, ecology and control of soil-transmitted helminth infections". Global Mapping of Infectious Diseases: Methods, Examples and Emerging Applications. Advances in Parasitology. Vol.62. pp.221–61. doi:10.1016/S0065-308X(05)62007-6. ISBN978-0120317622. PMC1976253. PMID16647972.{{cite book}}: |journal= ignored (help)
↑ Wallace, Barbara; Kirkley, James; McGuire, Thomas; Austin, Diane; Goldfield, David (April 2001). Assessment of Historical, Social, and Economic Impacts of OCS Development on Gulf Coast Communities(PDF) (Report). New Orleans: U .S. Department of the Interior. Bureau of Ocean Energy Management (BOEM), Minerals Management Service, Gulf of Mexico OCS Region. pp.35–36. Retrieved December 11, 2017. Inadequate public health services and a general lack of basic citizen knowledge of health and hygiene reflected the weak public education system. Health problems, especially in the Gulf Coast States where frost came late, if at all, abounded in an era when active public health departments in other parts of the country were eradicating nutritional and bacterial diseases. The hookworm, an intestinal parasite, infected and chronically debilitated a great many southerners, perhaps as many as 2 million. In the 1930s, a cooperative study by the Florida State Board of Health, the Rockefeller Foundation, and Vanderbilt University found the State's adolescents aged 15 to 18 the most affected group (44.7 percent), and the Panhandle the most severely affected area with nearly half of its teenagers (49 .2 percent) infested with hookworm (Eberson, 1980; and Link, 1988). John D. Rockefeller found the situation so appalling in the early twentieth century that he established and funded the Rockefeller Sanitary Commission for the Eradication of Hookworm Disease.
↑ Birn, Anne-Emanuelle; Solórzano, Armando (November 1999). "Public health policy paradoxes: science and politics in the Rockefeller Foundation's hookworm campaign in Mexico in the 1920s". Soc. Sci. Med. 49 (9): 1197–1213. doi:10.1016/S0277-9536(99)00160-4. PMID10501641.
↑ Spiegel A, Tall A, Raphenon G, Trape JF, Druilhe P (2003). "Increased frequency of malaria attacks in subjects co-infected by intestinal worms and Plasmodium falciparum malaria". Trans. R. Soc. Trop. Med. Hyg. 97 (2): 198–9. doi:10.1016/S0035-9203(03)90117-9. PMID14584377.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.