
Perspiration, also known as sweat, is the fluid secreted by sweat glands in the skin of mammals.
Irritation, in biology and physiology, is a state of inflammation or painful reaction to allergy or cell-lining damage. A stimulus or agent which induces the state of irritation is an irritant. Irritants are typically thought of as chemical agents but mechanical, thermal (heat), and radiative stimuli can also be irritants. Irritation also has non-clinical usages referring to bothersome physical or psychological pain or discomfort.

Sebaceous hyperplasia is a disorder of the sebaceous glands in which they become enlarged, producing flesh-colored or yellowish, shiny, often umbilicated bumps on the face. Newly formed nodules often swell with sweating, but this diminishes over time.

Tinea cruris, also known as jock itch, is a common type of contagious, superficial fungal infection of the groin and buttocks region, which occurs predominantly but not exclusively in men and in hot-humid climates.

Rosacea is a long-term skin condition that typically affects the face. It results in redness, pimples, swelling, and small and superficial dilated blood vessels. Often, the nose, cheeks, forehead, and chin are most involved. A red, enlarged nose may occur in severe disease, a condition known as rhinophyma.

Sweat glands, also known as sudoriferous or sudoriparous glands, from Latin sudor 'sweat', are small tubular structures of the skin that produce sweat. Sweat glands are a type of exocrine gland, which are glands that produce and secrete substances onto an epithelial surface by way of a duct. There are two main types of sweat glands that differ in their structure, function, secretory product, mechanism of excretion, anatomic distribution, and distribution across species:
Pityriasis rubra pilaris refers to a group of chronic disorders characterized by reddish orange, scaling plaques and keratotic follicular papules. Symptoms may include reddish-orange patches on the skin, severe flaking, uncomfortable itching, thickening of the skin on the feet and hands, and thickened bumps around hair follicles. For some, early symptoms may also include generalized swelling of the legs, feet and other parts of the body. PRP has a varied clinical progression and a varied rate of improvement. There is currently no known cause or cure for PRP.

Urushiol-induced contact dermatitis is a type of allergic contact dermatitis caused by the oil urushiol found in various plants, most notably sumac family species of the genus Toxicodendron: poison ivy, poison oak, poison sumac, and the Chinese lacquer tree. The name is derived from the Japanese word for the sap of the Chinese lacquer tree, urushi. Other plants in the sumac family also contain urushiol, as do unrelated plants such as Ginkgo biloba.

Polymorphous light eruption (PLE) presents with itchy red small bumps on sun-exposed skin, particularly face, neck, forearms and legs. It generally appears 30 minutes to a few hours after sun exposure and may last between one and 14 days. The bumps may become small blisters or plaques and may appear bloody,often healing with minimal scarring.

Perioral dermatitis, also known as periorificial dermatitis, is a common type of skin rash. Symptoms include multiple small (1–2 mm) bumps and blisters sometimes with background redness and scale, localized to the skin around the mouth and nostrils. Less commonly the eyes and genitalia may be involved. It can be persistent or recurring and resembles particularly rosacea and to some extent acne and allergic dermatitis. The term "dermatitis" is a misnomer because this is not an eczematous process.

Allergic contact dermatitis (ACD) is a form of contact dermatitis that is the manifestation of an allergic response caused by contact with a substance; the other type being irritant contact dermatitis (ICD).
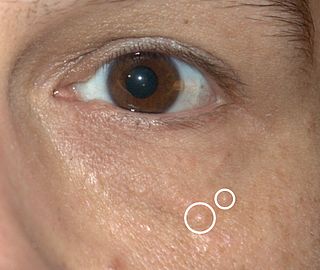
Syringomas are benign eccrine sweat duct tumors, typically found clustered on eyelids, although they may also be found in the armpits, abdomen, chest, neck, scalp, or groin area, including genitals, in a symmetric pattern. They are skin-colored or yellowish firm, rounded bumps, 1–3 mm in diameter, and may be confused with xanthoma, milia, hidrocystoma, trichoepithelioma, and xanthelasma. They are more common in women and are most commonly found in middle-aged Asian women. While they can present at any time in life, they typically present during adolescence. They are usually not associated with any other symptoms, although can sometimes cause itchiness or irritation.
Fox–Fordyce disease is a chronic blockage of the sweat gland ducts with a secondary, non-bacterial inflammatory response to the secretions and cellular debris in the cysts. The inflammation is often accompanied by intense itching. In general, the disease often causes skin to darken near the affected area and raised bumps or papules to appear. In addition, hair follicles can become damaged which cause hair loss. Hidradenitis is very similar, but tends to have a secondary bacterial infection so that pus-draining sinuses are formed. It is a very devastating skin disease that does not have universally curative treatments.

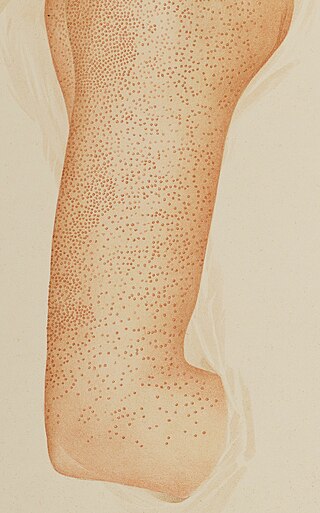
Cholinergic urticaria is a type of hives (urticaria) that is triggered by an increase in body temperature, such as during exercise, sweating, or exposure to heat. It is also sometimes called exercise-induced urticaria or heat hives. The condition is caused by an overreaction of the immune system to the release of histamine and other chemicals in response to the increase in body temperature. This results in the characteristic red, itchy, and sometimes raised bumps or welts on the skin that are associated with hives.
Hypohidrosis is a disorder in which a person exhibits diminished sweating in response to appropriate stimuli. In contrast with hyperhidrosis, which is a socially troubling yet often benign condition, the consequences of untreated hypohidrosis include hyperthermia, heat stroke and death. An extreme case of hypohidrosis in which there is a complete absence of sweating and the skin is dry is termed anhidrosis.

Heat illness is a spectrum of disorders due to increased body temperature. It can be caused by either environmental conditions or by exertion. It includes minor conditions such as heat cramps, heat syncope, and heat exhaustion as well as the more severe condition known as heat stroke. It can affect any or all anatomical systems. Heat illnesses include: heat stroke, heat exhaustion, heat syncope, heat edema, heat cramps, heat rash, heat tetany.
Acne mechanica is an acneiform eruption that has been observed after repetitive physical trauma to the skin such as rubbing, occurring from clothing or sports equipment. In addition to those mechanisms, the skin not getting enough exposure to air also contributes to the formation of acne mechanica. It is often mistaken as a rash that forms on sweaty skin that is constantly being rubbed, but in reality, it is a breakout of acne mechanica. The term "acne" itself describes the occurrence in which hair follicles in the skin get clogged by oil, dead skin cells, dirt and bacteria, or cosmetic products and create a pimple. Pimples can vary in type, size, and shape, but the sole basis of them occurring is the same - the oil gland in the pore becomes clogged and sometimes infected, which creates pus in order to fight the infection and subsequently causes the development of swollen, red lesions on the skin.

Superficial lymphatic malformation is a congenital malformation of the superficial lymphatics, presenting as groups of deep-seated, vesicle-like papules resembling frog spawn, at birth or shortly thereafter. Lymphangioma circumscriptum is the most common congenital lymphatic malformation. It is a benign condition and treatment is not required if the person who has it does not have symptoms from it.

Syringocystadenoma papilliferum is a rare non-malignant adnexal neoplasm that develops from apocrine or eccrine sweat glands and can be identified histologically by cystic, papillary, and ductal invaginations into the dermis lined by double-layered outer cuboidal and luminal high columnar epithelium and connected to the epidermis.
A coma blister, or coma bullae, is a skin lesion or blister that typically arises due to pressure in an individual with impaired consciousness. They vary in size, ranging from 4 to 5 centimeters in diameter, and may appear hemorrhagic or blood filled. Coma blisters are usually found in the extremities and trunk. These types of blisters have been associated with the overdose of central nervous system (CNS) depressants especially barbiturates, but also tricyclic antidepressants, hypnotics, benzodiazepines, opiates, antipsychotics, and alcohol. However, studies have found that coma blisters are not caused by the toxicity of these drugs, but due to hypoxia and external pressure on the comatose individual's skin from being immobilized. Coma blisters have been frequently found on individuals who have overdosed on drugs, but have also been found on individuals with chronic kidney failure, hypercalcemia, diabetic ketoacidosis, and a variety of neurologic conditions. Coma blisters are more frequent in adults and less common among children as demonstrated by the few cases published in literature.

