6% of babies (mouth)[7] 75% of women at some time (vaginal)[8]
Candidiasis is a fungal infection due to any species of the genus Candida (a yeast).[4] When it affects the mouth, in some countries it is commonly called thrush.[3] Signs and symptoms include white patches on the tongue or other areas of the mouth and throat.[3] Other symptoms may include soreness and problems swallowing.[9] When it affects the vagina, it may be referred to as a yeast infection or thrush.[2][10] Signs and symptoms include genital itching, burning, and sometimes a white "cottage cheese-like" discharge from the vagina.[11] Yeast infections of the penis are less common and typically present with an itchy rash.[11] Very rarely, yeast infections may become invasive, spreading to other parts of the body.[12] This may result in fevers, among other symptoms.[12]
More than 20 types of Candida may cause infection with Candida albicans being the most common.[13] Infections of the mouth are most common among children less than one month old, the elderly, and those with weak immune systems.[5] Conditions that result in a weak immune system include HIV/AIDS, the medications used after organ transplantation, diabetes, and the use of corticosteroids.[5] Other risk factors include during breastfeeding, following antibiotic therapy, and the wearing of dentures.[5][14] Vaginal infections occur more commonly during pregnancy, in those with weak immune systems, and following antibiotic therapy.[15] Individuals at risk for invasive candidiasis include low birth weight babies, people recovering from surgery, people admitted to intensive care units, and those with an otherwise compromised immune system.[16]
Efforts to prevent infections of the mouth include the use of chlorhexidine mouthwash in those with poor immune function and washing out the mouth following the use of inhaled steroids.[6] Little evidence supports probiotics for either prevention or treatment, even among those with frequent vaginal infections.[17][18] For infections of the mouth, treatment with topicalclotrimazole or nystatin is usually effective.[6] Oral or intravenous fluconazole, itraconazole, or amphotericin B may be used if these do not work.[6] A number of topical antifungal medications may be used for vaginal infections, including clotrimazole.[19] In those with widespread disease, an echinocandin such as caspofungin or micafungin is used.[20] A number of weeks of intravenous amphotericin B may be used as an alternative.[20] In certain groups at very high risk, antifungal medications may be used preventively,[16][20] and concomitantly with medications known to precipitate infections.
Infections of the mouth occur in about 6% of babies less than a month old.[7] About 20% of those receiving chemotherapy for cancer and 20% of those with AIDS also develop the disease.[7] About three-quarters of women have at least one yeast infection at some time during their lives.[8] Widespread disease is rare except in those who have risk factors.[21]
Signs and symptoms of candidiasis vary depending on the area affected.[22] Most candidal infections result in minimal complications such as redness, itching, and discomfort, though complications may be severe or even fatal if left untreated in certain populations. In healthy (immunocompetent) persons, candidiasis is usually a localized infection of the skin, fingernails or toenails (onychomycosis), or mucosal membranes, including the oral cavity and pharynx (thrush), esophagus, and the sex organs (vagina, penis, etc.);[23][24][25] less commonly in healthy individuals, the gastrointestinal tract,[26][27][28]urinary tract,[26] and respiratory tract[26] are sites of candida infection.
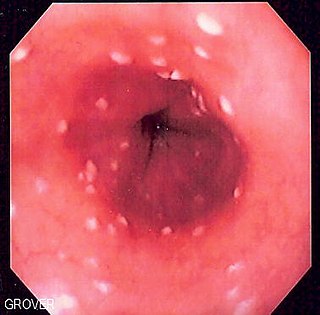
In immunocompromised individuals, Candida infections in the esophagus occur more frequently than in healthy individuals and have a higher potential of becoming systemic, causing a much more serious condition, a fungemia called candidemia.[23][29][30] Symptoms of esophageal candidiasis include difficulty swallowing, painful swallowing, abdominal pain, nausea, and vomiting.[23][31]
Mouth
Infection in the mouth is characterized by white discolorations in the tongue, around the mouth, and in the throat. Irritation may also occur, causing discomfort when swallowing.[32]
Thrush is commonly seen in infants. It is not considered abnormal in infants unless it lasts longer than a few weeks.[33]
Genitals
Infection of the vagina or vulva may cause severe itching, burning, soreness, irritation, and a whitish or whitish-gray cottage cheese-like discharge. Symptoms of infection of the male genitalia (balanitis thrush) include red skin around the head of the penis, swelling, irritation, itchiness and soreness of the head of the penis, thick, lumpy discharge under the foreskin, unpleasant odour, difficulty retracting the foreskin (phimosis), and pain when passing urine or during sex.[34]
Skin
Signs and symptoms of candidiasis in the skin include itching, irritation, and chafing or broken skin.[35]
Invasive infection
Common symptoms of gastrointestinal candidiasis in healthy individuals are anal itching, belching, bloating, indigestion, nausea, diarrhea, gas, intestinal cramps, vomiting, and gastric ulcers.[26][27][28] Perianal candidiasis can cause anal itching; the lesion can be red, papular, or ulcerative in appearance, and it is not considered to be a sexually transmitted infection.[36] Abnormal proliferation of the candida in the gut may lead to dysbiosis.[37] While it is not yet clear, this alteration may be the source of symptoms generally described as the irritable bowel syndrome,[38][39] and other gastrointestinal diseases.[27][40]
Neurological symptoms
Systemic candidiasis can affect the central nervous system causing a variety of neurological symptoms, with a presentation similar to meningitis.
Candida yeasts are generally present in healthy humans, frequently part of the human body's normal oral and intestinal flora, and particularly on the skin; however, their growth is normally limited by the human immune system and by competition of other microorganisms, such as bacteria occupying the same locations in the human body.[41]Candida requires moisture for growth, notably on the skin.[42] For example, wearing wet swimwear for long periods of time is believed to be a risk factor.[43] Candida can also cause diaper rashes in babies.[35] In extreme cases, superficial infections of the skin or mucous membranes may enter the bloodstream and cause systemic Candida infections.[citation needed]
Factors that increase the risk of candidiasis include HIV/AIDS, mononucleosis, cancer treatments, steroids, stress, antibiotic therapy, diabetes, and nutrient deficiency. Hormone replacement therapy and infertility treatments may also be predisposing factors.[44] Use of inhaled corticosteroids increases risk of candidiasis of the mouth.[45] Inhaled corticosteroids with other risk factors such as antibiotics, oral glucocorticoids, not rinsing mouth after use of inhaled corticosteroids or high dose of inhaled corticosteroids put people at even higher risk.[45] Treatment with antibiotics can lead to eliminating the yeast's natural competitors for resources in the oral and intestinal flora, thereby increasing the severity of the condition.[46] A weakened or undeveloped immune system or metabolic illnesses are significant predisposing factors of candidiasis.[47] Almost 15% of people with weakened immune systems develop a systemic illness caused by Candida species.[48] Diets high in simple carbohydrates have been found to affect rates of oral candidiases.[49]
C. albicans was isolated from the vaginas of 19% of apparently healthy women, i.e., those who experienced few or no symptoms of infection. External use of detergents or douches or internal disturbances (hormonal or physiological) can perturb the normal vaginal flora, consisting of lactic acid bacteria, such as lactobacilli, and result in an overgrowth of Candida cells, causing symptoms of infection, such as local inflammation.[50] Pregnancy and the use of oral contraceptives have been reported as risk factors.[51]Diabetes mellitus and the use of antibiotics are also linked to increased rates of yeast infections.[51]
In penile candidiasis, the causes include sexual intercourse with an infected individual, low immunity, antibiotics, and diabetes. Male genital yeast infections are less common, but a yeast infection on the penis caused from direct contact via sexual intercourse with an infected partner is not uncommon.[52]
Breast-feeding mothers may also develop candidiasis on and around the nipple as a result of moisture created by excessive milk-production.[14]
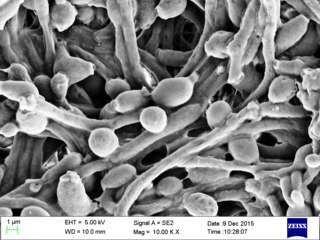
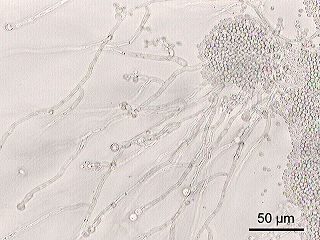
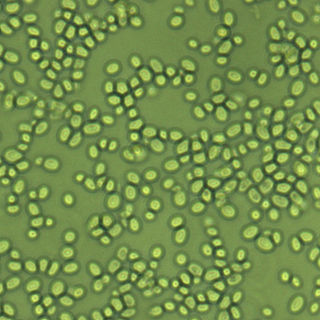
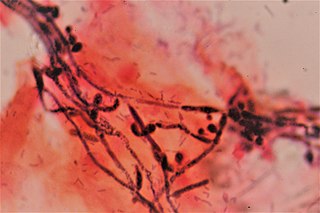
Vaginal swab wet mount of candida (phase contrast) showing the pseudohyphaeAgar plate culture of C. albicansKOH test on a vaginal wet mount, showing slings of pseudohyphae of Candida albicans surrounded by round vaginal epithelial cells, conferring a diagnosis of candidal vulvovaginitisMicrograph of esophageal candidiasis showing hyphae, biopsy specimen, PAS stainGram stain of Candida albicans from a vaginal swab; the small oval chlamydospores are 2–4μm in diameter Chromogenic agar can help in indicating the involved species of Candida versus similar fungi. (CHROMAgar shown)
In oral candidiasis, simply inspecting the person's mouth for white patches and irritation may make the diagnosis. A sample of the infected area may also be taken to determine what organism is causing the infection.[54]
Symptoms of vaginal candidiasis are also present in the more common bacterial vaginosis;[55] aerobic vaginitis is distinct and should be excluded in the differential diagnosis.[56] In a 2002 study, only 33% of women who were self-treating for a yeast infection were found to have such an infection, while most had either bacterial vaginosis or a mixed-type infection.[57]
Diagnosis of a yeast infection is confirmed either via microscopic examination or culturing. For identification by light microscopy, a scraping or swab of the affected area is placed on a microscope slide. A single drop of 10% potassium hydroxide (KOH) solution is then added to the specimen. The KOH dissolves the skin cells, but leaves the Candida cells intact, permitting visualization of pseudohyphae and budding yeast cells typical of many Candida species.[citation needed]
For the culturing method, a sterile swab is rubbed on the infected skin surface. The swab is then streaked on a culture medium. The culture is incubated at 37°C (98.6°F) for several days, to allow development of yeast or bacterial colonies. The characteristics (such as morphology and colour) of the colonies may allow initial diagnosis of the organism causing disease symptoms.[58] Respiratory, gastrointestinal, and esophageal candidiasis require an endoscopy to diagnose.[28][59] For gastrointestinal candidiasis, it is necessary to obtain a 3–5milliliter sample of fluid from the duodenum for fungal culture.[28] The diagnosis of gastrointestinal candidiasis is based upon the culture containing in excess of 1,000 colony-forming units per milliliter.[28]
A diet that supports the immune system and is not high in simple carbohydrates contributes to a healthy balance of the oral and intestinal flora.[41][49] While yeast infections are associated with diabetes, the level of blood sugar control may not affect the risk.[64] Wearing cotton underwear may help to reduce the risk of developing skin and vaginal yeast infections, along with not wearing wet clothes for long periods of time.[15][43] For women who experience recurrent yeast infections, there is limited evidence that oral or intravaginal probiotics help to prevent future infections.[17][65] This includes either as pills or as yogurt.[17]
Oral hygiene can help prevent oral candidiasis when people have a weakened immune system.[5] For people undergoing cancer treatment, chlorhexidine mouthwash can prevent or reduce thrush.[5] People who use inhaled corticosteroids can reduce the risk of developing oral candidiasis by rinsing the mouth with water or mouthwash after using the inhaler.[5] People with dentures should also disinfect their dentures regularly to prevent oral candidiasis.[54]
The 2016 revision of the clinical practice guideline for the management of candidiasis lists a large number of specific treatment regimens for Candida infections that involve different Candida species, forms of antifungal drug resistance, immune statuses, and infection localization and severity.[20] Gastrointestinal candidiasis in immunocompetent individuals is treated with 100–200mg fluconazole per day for 2–3weeks.[28]
Localized infection
Mouth and throat candidiasis are treated with antifungal medication. Oral candidiasis usually responds to topical treatments; otherwise, systemic antifungal medication may be needed for oral infections. Candidal skin infections in the skin folds (candidal intertrigo) typically respond well to topical antifungal treatments (e.g., nystatin or miconazole). For breastfeeding mothers topical miconazole is the most effective treatment for treating candidiasis on the breasts.[66]Gentian violet can be used for thrush in breastfeeding babies.[14] Systemic treatment with antifungals by mouth is reserved for severe cases or if treatment with topical therapy is unsuccessful. Candida esophagitis may be treated orally or intravenously; for severe or azole-resistant esophageal candidiasis, treatment with amphotericin B may be necessary.[6]
Vaginal yeast infections are typically treated with topical antifungal agents.[20] Penile yeast infections are also treated with antifungal agents, but while an internal treatment may be used (such as a pessary) for vaginal yeast infections, only external treatments– such as a cream– can be recommended for penile treatment.[67] A one-time dose of fluconazole by mouth is 90% effective in treating a vaginal yeast infection.[68] For severe nonrecurring cases, several doses of fluconazole is recommended.[20] Local treatment may include vaginal suppositories or medicated douches. Other types of yeast infections require different dosing. C. albicans can develop resistance to fluconazole, this being more of an issue in those with HIV/AIDS who are often treated with multiple courses of fluconazole for recurrent oral infections.[69]
For vaginal yeast infection in pregnancy, topical imidazole or triazole antifungals are considered the therapy of choice owing to available safety data.[70] Systemic absorption of these topical formulations is minimal, posing little risk of transplacental transfer.[70] In vaginal yeast infection in pregnancy, treatment with topical azole antifungals is recommended for seven days instead of a shorter duration.[70]
For vaginal yeast infections, many complementary treatments are proposed, however a number have side effects.[71] No benefit from probiotics has been found for active infections.[18]
In hospitalized patients who develop candidemia, age is an important prognostic factor. Mortality following candidemia is 50% in patients aged ≥75 years and 24% in patients aged <75 years.[73] Among individuals being treated in intensive care units, the mortality rate is about 30–50% when systemic candidiasis develops.[74]
Epidemiology
Oral candidiasis is the most common fungal infection of the mouth,[75] and it also represents the most common opportunistic oral infection in humans.[76] Infections of the mouth occur in about 6% of babies less than a month old.[7] About 20% of those receiving chemotherapy for cancer and 20% of those with AIDS also develop the disease.[7]
It is estimated that 20% of women may be asymptomatically colonized by vaginal yeast.[77] In the United States there are approximately 1.4 million doctor office visits every year for candidiasis.[78] About three-quarters of women have at least one yeast infection at some time during their lives.[8]
Esophageal candidiasis is the most common esophageal infection in persons with AIDS and accounts for about 50% of all esophageal infections, often coexisting with other esophageal diseases. About two-thirds of people with AIDS and esophageal candidiasis also have oral candidiasis.[31]
Candidal sepsis is rare.[79] Candida is the fourth most common cause of bloodstream infections among hospital patients in the United States.[80] The incidence of bloodstream candida in intensive care units varies widely between countries.[81]
History
Descriptions of what sounds like oral thrush go back to the time of Hippocratescirca 460–370 BCE.[22]
The first description of a fungus as the causative agent of an oropharyngeal and oesophageal candidosis was by Bernhard von Langenbeck in 1839.[82]
Vulvovaginal candidiasis was first described in 1849 by Wilkinson.[83] In 1875, Haussmann demonstrated the causative organism in both vulvovaginal and oral candidiasis is the same.[83]
With the advent of antibiotics following World War II, the rates of candidiasis increased. The rates then decreased in the 1950s following the development of nystatin.[84]
The colloquial term "thrush" refers to the resemblance of the white flecks present in some forms of candidiasis (e.g., pseudomembranous candidiasis) with the breast of the bird of the same name.[85] The term candidosis is largely used in British English, and candidiasis in American English.[83]Candida is also pronounced differently; in American English, the stress is on the "i", whereas in British English the stress is on the first syllable.[citation needed]
The genusCandida and speciesC. albicans were described by botanist Christine Marie Berkhout in her doctoral thesis at the University of Utrecht in 1923. Over the years, the classification of the genera and species has evolved. Obsolete names for this genus include Mycotorula and Torulopsis. The species has also been known in the past as Monilia albicans and Oidium albicans. The current classification is nomen conservandum, which means the name is authorized for use by the International Botanical Congress (IBC).[86]
The genus Candida includes about 150 different species. However, only a few are known to cause human infections. C. albicans is the most significant pathogenic species. Other species pathogenic in humans include C. auris, C. tropicalis, C. parapsilosis, C. dubliniensis, and C. lusitaniae.
The name Candida was proposed by Berkhout. It is from the Latin word toga candida, referring to the white toga (robe) worn by candidates for the Senate of the ancient Roman republic.[83] The specific epithet albicans also comes from Latin, albicare meaning "to whiten".[83] These names refer to the generally white appearance of Candida species when cultured.
A 2005 publication noted that "a large pseudoscientific cult"[87] has developed around the topic of Candida, with claims stating that up to one in three people are affected by yeast-related illness, particularly a condition called "Candidiasis hypersensitivity".[88] Some practitioners of alternative medicine have promoted these purported conditions and sold dietary supplements as supposed cures; a number of them have been prosecuted.[88][89] In 1990, alternative health vendor Nature's Way signed an FTC consent agreement not to misrepresent in advertising any self-diagnostic test concerning yeast conditions or to make any unsubstantiated representation concerning any food or supplement's ability to control yeast conditions, with a fine of $30,000 payable to the National Institutes of Health for research in genuine candidiasis.[89]
Research
High level Candida colonization is linked to several diseases of the gastrointestinal tract including Crohn's disease.[90][91]
There has been an increase in resistance to antifungals worldwide over the past 30–40 years.[92][93]
Related Research Articles
Vaginitis, also known as vulvovaginitis, is inflammation of the vagina and vulva. Symptoms may include itching, burning, pain, discharge, and a bad smell. Certain types of vaginitis may result in complications during pregnancy.
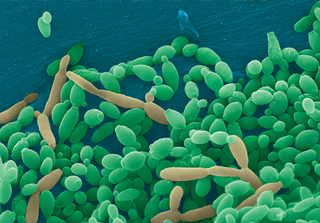
Candida albicans is an opportunistic pathogenic yeast that is a common member of the human gut flora. It can also survive outside the human body. It is detected in the gastrointestinal tract and mouth in 40–60% of healthy adults. It is usually a commensal organism, but it can become pathogenic in immunocompromised individuals under a variety of conditions. It is one of the few species of the genus Candida that cause the human infection candidiasis, which results from an overgrowth of the fungus. Candidiasis is, for example, often observed in HIV-infected patients. C. albicans is the most common fungal species isolated from biofilms either formed on (permanent) implanted medical devices or on human tissue. C. albicans, C. tropicalis, C. parapsilosis, and C. glabrata are together responsible for 50–90% of all cases of candidiasis in humans. A mortality rate of 40% has been reported for patients with systemic candidiasis due to C. albicans. By one estimate, invasive candidiasis contracted in a hospital causes 2,800 to 11,200 deaths yearly in the US. Nevertheless, these numbers may not truly reflect the true extent of damage this organism causes, given new studies indicating that C. albicans can cross the blood–brain barrier in mice.
Candida is a genus of yeasts. It is the most common cause of fungal infections worldwide and the largest genus of medically important yeast.
Fluconazole is an antifungal medication used for a number of fungal infections. This includes candidiasis, blastomycosis, coccidioidomycosis, cryptococcosis, histoplasmosis, dermatophytosis, and tinea versicolor. It is also used to prevent candidiasis in those who are at high risk such as following organ transplantation, low birth weight babies, and those with low blood neutrophil counts. It is given either by mouth or by injection into a vein.
Oral candidiasis (Acute pseudomembranous candidiasis), also known as oral thrush among other names, is candidiasis that occurs in the mouth. That is, oral candidiasis is a mycosis (yeast/fungal infection) of Candida species on the mucous membranes of the mouth.
Fungal infection, also known as mycosis, is a disease caused by fungi. Different types are traditionally divided according to the part of the body affected; superficial, subcutaneous, and systemic. Superficial fungal infections include common tinea of the skin, such as tinea of the body, groin, hands, feet and beard, and yeast infections such as pityriasis versicolor. Subcutaneous types include eumycetoma and chromoblastomycosis, which generally affect tissues in and beneath the skin. Systemic fungal infections are more serious and include cryptococcosis, histoplasmosis, pneumocystis pneumonia, aspergillosis and mucormycosis. Signs and symptoms range widely. There is usually a rash with superficial infection. Fungal infection within the skin or under the skin may present with a lump and skin changes. Pneumonia-like symptoms or meningitis may occur with a deeper or systemic infection.
Terconazole is an antifungal drug used to treat vaginal yeast infection. It comes as a lotion or a suppository and disrupts the biosynthesis of fats in a yeast cell. It has a relatively broad spectrum compared to azole compounds but not triazole compounds. Testing shows that it is a suitable compound for prophylaxis for those that suffer from chronic vulvovaginal candidiasis.
Fungemia is the presence of fungi or yeast in the blood. The most common type, also known as candidemia, candedemia, or systemic candidiasis, is caused by Candida species. Candidemia is also among the most common bloodstream infections of any kind. Infections by other fungi, including Saccharomyces, Aspergillus and Cryptococcus, are also called fungemia. It is most commonly seen in immunosuppressed or immunocompromised patients with severe neutropenia, cancer patients, or in patients with intravenous catheters. It has been suggested that otherwise immunocompetent patients taking infliximab may also be at a higher risk.
Candida parapsilosis is a fungal species of yeast that has become a significant cause of sepsis and of wound and tissue infections in immunocompromised people. Unlike Candida albicans and Candida tropicalis, C. parapsilosis is not an obligate human pathogen, having been isolated from nonhuman sources such as domestic animals, insects and soil. C. parapsilosis is also a normal human commensal and it is one of the fungi most frequently isolated from human hands. There are several risk factors that can contribute to C. parapsilosis colonization. Immunocompromised individuals and surgical patients, particularly those undergoing surgery of the gastrointestinal tract, are at high risk for infection with C. parapsilosis. There is currently no consensus on the treatment of invasive candidiasis caused by C. parapsilosis, although the therapeutic approach typically includes the removal of foreign bodies such as implanted prostheses and the administration of systemic antifungal therapy. Amphotericin B and Fluconazole are often used in the treatment of C. parapsilosis infection.
Nakaseomyces glabratus is a species of haploid yeast of the genus Nakaseomyces, previously known as Candida glabrata. Despite the fact that no sexual life cycle has been documented for this species, N. glabratus strains of both mating types are commonly found. N. glabrata is generally a commensal of human mucosal tissues, but in today's era of wider human immunodeficiency from various causes, N. glabratus is often the second or third most common cause of candidiasis as an opportunistic pathogen. Infections caused by N. glabratus can affect the urogenital tract or even cause systemic infections by entrance of the fungal cells in the bloodstream (Candidemia), especially prevalent in immunocompromised patients.
Esophageal candidiasis is an opportunistic infection of the esophagus by Candida albicans. The disease usually occurs in patients in immunocompromised states, including post-chemotherapy and in AIDS. However, it can also occur in patients with no predisposing risk factors, and is more likely to be asymptomatic in those patients. It is also known as candidal esophagitis or monilial esophagitis.
Echinocandins are a class of antifungal drugs that inhibit the synthesis of β-glucan in the fungal cell wall via noncompetitive inhibition of the enzyme 1,3-β glucan synthase. The class has been termed the "penicillin of antifungals," along with the related papulacandins, as their mechanism of action resembles that of penicillin in bacteria. β-glucans are carbohydrate polymers that are cross-linked with other fungal cell wall components, the fungal equivalent to bacterial peptidoglycan. Caspofungin, micafungin, and anidulafungin are semisynthetic echinocandin derivatives with limited clinical use due to their solubility, antifungal spectrum, and pharmacokinetic properties.
Fenticonazole is an imidazole antifungal drug, used locally as the nitrate in the treatment of vulvovaginal candidiasis. It is active against a range of organisms including dermatophyte pathogens, Malassezia furfur, and Candida albicans. Fenticonazole has also been shown to exhibit antibacterial action, with a spectrum of activity that includes bacteria commonly associated with superinfected fungal skin and vaginal infections, and antiparasitic action against the protozoan Trichomonas vaginalis.
Clotrimazole, sold under the brand name Lotrimin, among others, is an antifungal medication. It is used to treat vaginal yeast infections, oral thrush, diaper rash, tinea versicolor, and types of ringworm including athlete's foot and jock itch. It can be taken by mouth or applied as a cream to the skin or in the vagina.
Vaginal yeast infection, also known as candidal vulvovaginitis and vaginal thrush, is excessive growth of yeast in the vagina that results in irritation. The most common symptom is vaginal itching, which may be severe. Other symptoms include burning with urination, a thick, white vaginal discharge that typically does not smell bad, pain during sex, and redness around the vagina. Symptoms often worsen just before a woman's period.
Invasive candidiasis is an infection (candidiasis) that can be caused by various species of Candida yeast. Unlike Candida infections of the mouth and throat or vagina, invasive candidiasis is a serious, progressive, and potentially fatal infection that can affect the blood (fungemia), heart, brain, eyes, bones, and other parts of the body.
Candida tropicalis is a species of yeast in the genus Candida. It is a common pathogen in neutropenic hosts, in whom it may spread through the bloodstream to peripheral organs. For invasive disease, treatments include amphotericin B, echinocandins, or extended-spectrum triazole antifungals.
Ibrexafungerp, sold under the brand name Brexafemme, is an antifungal medication used to treat vulvovaginal candidiasis (VVC). It is taken orally. It is also currently undergoing clinical trials for other indications via an intravenous (IV) formulation. An estimated 75% of women will have at least one episode of VVC and 40 to 45% will have two or more episodes in their lifetime.
Topical antifungaldrugs are used to treat fungal infections on the skin, scalp, nails, vagina or inside the mouth. These medications come as creams, gels, lotions, ointments, powders, shampoos, tinctures and sprays. Most antifungal drugs induce fungal cell death by destroying the cell wall of the fungus. These drugs inhibit the production of ergosterol, which is a fundamental component of the fungal cell membrane and wall.
Oteseconazole, a novel orally bioavailable and selective inhibitor of fungal cytochrome P450 enzyme 51 (CYP51), has shown promising efficacy in the treatment of recurrent vulvovaginal candidiasis (RVVC) in patients.
References
1 2 3 James WD, Elston DM, Berger TG, Andrews GC, etal. (2006). Andrews' Diseases of the Skin: clinical Dermatology. Saunders Elsevier. pp.308–311. ISBN978-0-7216-2921-6.
1 2 "Vaginal Candidiasis". Fungal Diseases. United States: Centers for Disease Control and Prevention. 13 November 2019. Archived from the original on 29 December 2014. Retrieved 24 Dec 2019.
1 2 "Candidiasis". Fungal Diseases. United States: Centers for Disease Control and Prevention. 13 November 2019. Archived from the original on 29 December 2014. Retrieved 24 Dec 2019.
1 2 3 Jurden L, Buchanan M, Kelsberg G, Safranek S (June 2012). "Clinical inquiries. Can probiotics safely prevent recurrent vaginitis?". The Journal of Family Practice. 61 (6): 357, 368. PMID22670239.
1 2 Abad CL, Safdar N (June 2009). "The role of lactobacillus probiotics in the treatment or prevention of urogenital infections--a systematic review". Journal of Chemotherapy. 21 (3): 243–52. doi:10.1179/joc.2009.21.3.243. PMID19567343. S2CID32398416.
1 2 Dolin GL, Mandell JE, Bennett R (2010). Mandell, Douglas, and Bennett's principles and practice of infectious diseases (7thed.). Philadelphia, PA: Churchill Livingstone/Elsevier. pp.Chapter 250. ISBN978-0-443-06839-3.
1 2 3 4 5 6 Martins N, Ferreira IC, Barros L, Silva S, Henriques M (June 2014). "Candidiasis: predisposing factors, prevention, diagnosis and alternative treatment"(PDF). Mycopathologia. 177 (5–6): 223–40. doi:10.1007/s11046-014-9749-1. hdl:10198/10147. PMID24789109. S2CID795450. Archived(PDF) from the original on 2017-08-17. Retrieved 2019-09-24. Candida species and other microorganisms are involved in this complicated fungal infection, but Candida albicans continues to be the most prevalent. In the past two decades, it has been observed an abnormal overgrowth in the gastrointestinal, urinary and respiratory tracts, not only in immunocompromised patients but also related to nosocomial infections and even in healthy individuals. There is a wide variety of causal factors that contribute to yeast infection which means that candidiasis is a good example of a multifactorial syndrome.
1 2 3 4 Wang ZK, Yang YS, Stefka AT, Sun G, Peng LH (April 2014). "Review article: fungal microbiota and digestive diseases". Alimentary Pharmacology & Therapeutics. 39 (8): 751–66. doi:10.1111/apt.12665. PMID24612332. S2CID22101484. In addition, GI fungal infection is reported even among those patients with normal immune status. Digestive system-related fungal infections may be induced by both commensal opportunistic fungi and exogenous pathogenic fungi. The IFI in different GI sites have their special clinical features, which are often accompanied by various severe diseases. Although IFI associated with digestive diseases are less common, they can induce fatal outcomes due to less specificity of related symptoms, signs, endoscopic and imaging manifestations, and the poor treatment options.... Candida sp. is also the most frequently identified species among patients with gastric IFI.... Gastric IFI is often characterised by the abdominal pain and vomiting and with the endoscopic characteristics including gastric giant and multiple ulcers, stenosis, perforation, and fistula. For example, gastric ulcers combined with entogastric fungal infection, characterised by deep, large and intractable ulcers,[118] were reported as early as the 1930s.... The overgrowth and colonisation of fungi in intestine can lead to diarrhoea.
1 2 3 4 5 6 7 Erdogan A, Rao SS (April 2015). "Small intestinal fungal overgrowth". Current Gastroenterology Reports. 17 (4): 16. doi:10.1007/s11894-015-0436-2. PMID25786900. S2CID3098136. Small intestinal fungal overgrowth (SIFO) is characterized by the presence of excessive number of fungal organisms in the small intestine associated with gastrointestinal (GI) symptoms. Candidiasis is known to cause GI symptoms particularly in immunocompromised patients or those receiving steroids or antibiotics. However, only recently, there is emerging literature that an overgrowth of fungus in the small intestine of non-immunocompromised subjects may cause unexplained GI symptoms. Two recent studies showed that 26% (24/94) and 25.3% (38/150) of a series of patients with unexplained GI symptoms had SIFO. The most common symptoms observed in these patients were belching, bloating, indigestion, nausea, diarrhea, and gas. The underlying mechanism(s) that predisposes to SIFO is unclear but small intestinal dysmotility and use of proton pump inhibitors has been implicated. However, further studies are needed; both to confirm these observations and to examine the clinical relevance of fungal overgrowth, both in healthy subjects and in patients with otherwise unexplained GI symptoms.... For routine SIFO in an immunocompetent host, a 2–3 week oral course of fluconazole 100–200 mg will suffice.
1 2 Skoczylas MM, Walat A, Kordek A, Loniewska B, Rudnicki J, Maleszka R, etal. (2014). "Congenital candidiasis as a subject of research in medicine and human ecology". Annals of Parasitology. 60 (3): 179–89. PMID25281815.
↑ Nolting S, Brautigam M, Weidinger G (April 1994). "Terbinafine in onychomycosis with involvement by non-dermatophytic fungi". The British Journal of Dermatology. 130 (Suppl 43): 16–21. doi:10.1111/j.1365-2133.1994.tb06088.x. PMID8186136. S2CID37415499.
↑ Reiss E, Shadomy HJ, Lyon GM (2011). "Chapter 11". Fundamental medical mycology. Hoboken, N.J.: John Wiley & Sons. ISBN978-1-118-10176-6. Archived from the original on 2016-04-30.
↑ Felix TC, de Brito Röder DV, Dos Santos Pedroso R (March 2019). "Alternative and complementary therapies for vulvovaginal candidiasis". Folia Microbiologica. 64 (2): 133–141. doi:10.1007/s12223-018-0652-x. PMID30269301. S2CID52889140.
↑ "Systemic candidiasis". NIH.gov. U.S. DHHS, National Institute of Health. Oct 2014. Archived from the original on April 27, 2015. Retrieved April 19, 2015.
↑ "Candida"(PDF). CDC.gov. Center of Disease Control. Archived(PDF) from the original on April 27, 2015. Retrieved April 19, 2015.
↑ Vallabhaneni S, Mody RK, Walker T, Chiller T (2016). "1. The global burden of fungal disease". In Sobel J, Ostrosky-Zeichner L (eds.). Fungal Infections, An Issue of Infectious Disease Clinics of North America. Philadelphia: Elsevier. pp.2–3. ISBN978-0-323-41649-8. Archived from the original on 2024-02-24. Retrieved 2021-05-29.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.