
Systemic scleroderma, or systemic sclerosis, is an autoimmune rheumatic disease characterised by excessive production and accumulation of collagen, called fibrosis, in the skin and internal organs and by injuries to small arteries. There are two major subgroups of systemic sclerosis based on the extent of skin involvement: limited and diffuse. The limited form affects areas below, but not above, the elbows and knees with or without involvement of the face. The diffuse form also affects the skin above the elbows and knees and can also spread to the torso. Visceral organs, including the kidneys, heart, lungs, and gastrointestinal tract can also be affected by the fibrotic process. Prognosis is determined by the form of the disease and the extent of visceral involvement. Patients with limited systemic sclerosis have a better prognosis than those with the diffuse form. Death is most often caused by lung, heart, and kidney involvement. The risk of cancer is increased slightly.

Sjögren syndrome or Sjögren's syndrome is a long-term autoimmune disease that affects the body's moisture-producing glands, and often seriously affects other organ systems, such as the lungs, kidneys, and nervous system.

In immunology, autoimmunity is the system of immune responses of an organism against its own healthy cells, tissues and other normal body constituents. Any disease resulting from this type of immune response is termed an "autoimmune disease". Prominent examples include celiac disease, diabetes mellitus type 1, Henoch–Schönlein purpura, systemic lupus erythematosus, Sjögren syndrome, eosinophilic granulomatosis with polyangiitis, Hashimoto's thyroiditis, Graves' disease, idiopathic thrombocytopenic purpura, Addison's disease, rheumatoid arthritis, ankylosing spondylitis, polymyositis, dermatomyositis, and multiple sclerosis. Autoimmune diseases are very often treated with steroids.
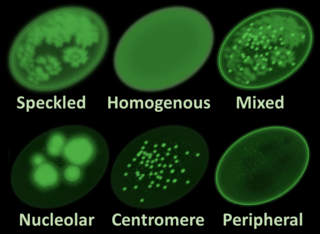
Antinuclear antibodies are autoantibodies that bind to contents of the cell nucleus. In normal individuals, the immune system produces antibodies to foreign proteins (antigens) but not to human proteins (autoantigens). In some cases, antibodies to human antigens are produced.

Raynaud syndrome, also known as Raynaud's phenomenon, is a medical condition in which the spasm of small arteries causes episodes of reduced blood flow to end arterioles. Typically, the fingers, and less commonly, the toes, are involved. Rarely, the nose, ears, nipples, or lips are affected. The episodes classically result in the affected part turning white and then blue. Often, numbness or pain occurs. As blood flow returns, the area turns red and burns. The episodes typically last minutes but can last several hours. The condition is named after the physician Auguste Gabriel Maurice Raynaud, who first described it in his doctoral thesis in 1862.

CREST syndrome, also known as the limited cutaneous form of systemic sclerosis (lcSSc), is a multisystem connective tissue disorder. The acronym "CREST" refers to the five main features: calcinosis, Raynaud's phenomenon, esophageal dysmotility, sclerodactyly, and telangiectasia.

Morphea is a form of scleroderma that mainly involves isolated patches of hardened skin on the face, hands, and feet, or anywhere else on the body, usually with no internal organ involvement. However, in Deep Morphea inflammation and sclerosis can be found in the deep dermis, panniculus, fascia, superficial muscle and bone.
Mixed connective tissue disease, commonly abbreviated as MCTD, is an autoimmune disease characterized by the presence of elevated blood levels of a specific autoantibody, now called anti-U1 ribonucleoprotein (RNP), together with a mix of symptoms of systemic lupus erythematosus (SLE), scleroderma, and polymyositis. The idea behind the "mixed" disease is that this specific autoantibody is also present in other autoimmune diseases such as systemic lupus erythematosus, polymyositis, scleroderma, etc. MCTD was characterized as an individual disease in 1972 by Sharp et al., and the term was introduced by Leroy in 1980.
Type V collagen is a form of fibrillar collagen associated with classical Ehlers-Danlos syndrome. It is found within the dermal/epidermal junction, placental tissues, as well as in association with tissues containing type I collagen.
Scleromyositis, is an autoimmune disease. People with scleromyositis have symptoms of both systemic scleroderma and either polymyositis or dermatomyositis, and is therefore considered an overlap syndrome. Although it is a rare disease, it is one of the more common overlap syndromes seen in scleroderma patients, together with MCTD and Antisynthetase syndrome. Autoantibodies often found in these patients are the anti-PM/Scl (anti-exosome) antibodies.
An overlap syndrome is a medical condition which shares features of at least two more widely recognised disorders. Examples of overlap syndromes can be found in many medical specialties such as overlapping connective tissue disorders in rheumatology, and overlapping genetic disorders in cardiology.
Anti-topoisomerase antibodies (ATA) are autoantibodies directed against topoisomerase and found in several diseases, most importantly scleroderma. Diseases with ATA are autoimmune disease because they react with self-proteins. They are also referred to as anti-DNA topoisomerase I antibody.

Autoimmune inner ear disease (AIED) was first defined by Dr. Brian McCabe in a landmark paper describing an autoimmune loss of hearing. The disease results in progressive sensorineural hearing loss (SNHL) that acts bilaterally and asymmetrically, and sometimes affects an individual's vestibular system. AIED is used to describe any disorder in which the inner ear is damaged as a result of an autoimmune response. Some examples of autoimmune disorders that have presented with AIED are Cogan's syndrome, relapsing polychondritis, systemic lupus erythematosus, granulomatosis with polyangiitis, polyarteritis nodosa, Sjogren's syndrome, and Lyme disease.

An autoimmune disease is a condition that results from an anomalous response of the adaptive immune system, wherein it mistakenly targets and attacks healthy, functioning parts of the body as if they were foreign organisms. It is estimated that there are more than 80 recognized autoimmune diseases, with recent scientific evidence suggesting the existence of potentially more than 100 distinct conditions. Nearly any body part can be involved.

Necrotizing vasculitis, also called systemic necrotizing vasculitis, is a general term for the inflammation of veins and arteries that develops into necrosis and narrows the vessels.
Lupus, technically known as systemic lupus erythematosus (SLE), is an autoimmune disease in which the body's immune system mistakenly attacks healthy tissue in many parts of the body. Symptoms vary among people and may be mild to severe. Common symptoms include painful and swollen joints, fever, chest pain, hair loss, mouth ulcers, swollen lymph nodes, feeling tired, and a red rash which is most commonly on the face. Often there are periods of illness, called flares, and periods of remission during which there are few symptoms.
Undifferentiated connective tissue disease (UCTD) is a disease in which the connective tissues are targeted by the immune system. It is a serological and clinical manifestation of an autoimmune disease. When there is proof of an autoimmune disease, it will be diagnosed as UCTD if the disease doesn't answer to any criterion of specific autoimmune disease. This is also the case of major rheumatic diseases whose early phase was defined by LeRoy et al. in 1980 as undifferentiated connective tissue disease.

Anti-SSA autoantibodies are a type of anti-nuclear autoantibodies that are associated with many autoimmune diseases, such as systemic lupus erythematosus (SLE), SS/SLE overlap syndrome, subacute cutaneous lupus erythematosus (SCLE), neonatal lupus and primary biliary cirrhosis. They are often present in Sjögren's syndrome (SS). Additionally, Anti-Ro/SSA can be found in other autoimmune diseases such as systemic sclerosis (SSc), polymyositis/dermatomyositis (PM/DM), rheumatoid arthritis (RA), and mixed connective tissue disease (MCTD), and are also associated with heart arrhythmia.
Autoimmunity refers to a pathological immune response of the body's immune system against itself. Autoimmune disease is widely recognized to be significantly more common in women than in men, and often presents differently between the sexes. The reasons for these disparities are still under investigation, but may in part involve the presence of an additional X chromosome in women, as well as the higher presence of female sex hormones such as estrogen. The risk, incidence, and character of autoimmune disease in women may also be associated with female-specific physiological changes, such as hormonal shifts during menses, pregnancy, and menopause.


