
Stevens–Johnson syndrome (SJS) is a type of severe skin reaction. Together with toxic epidermal necrolysis (TEN) and Stevens–Johnson/toxic epidermal necrolysis (SJS/TEN), it forms a spectrum of disease, with SJS being less severe. Erythema multiforme (EM) is generally considered a separate condition. Early symptoms of SJS include fever and flu-like symptoms. A few days later, the skin begins to blister and peel, forming painful raw areas. Mucous membranes, such as the mouth, are also typically involved. Complications include dehydration, sepsis, pneumonia and multiple organ failure.

A mouth ulcer (aphtha) is an ulcer that occurs on the mucous membrane of the oral cavity. Mouth ulcers are very common, occurring in association with many diseases and by many different mechanisms, but usually there is no serious underlying cause. Rarely, a mouth ulcer that does not heal may be a sign of oral cancer. These ulcers may form individually or multiple ulcers may appear at once. Once formed, an ulcer may be maintained by inflammation and/or secondary infection.

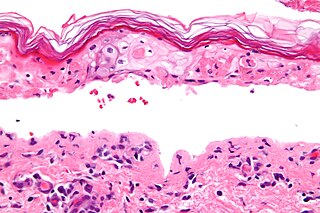
Toxic epidermal necrolysis (TEN) is a type of severe skin reaction. Together with Stevens–Johnson syndrome (SJS) it forms a spectrum of disease, with TEN being more severe. Early symptoms include fever and flu-like symptoms. A few days later the skin begins to blister and peel forming painful raw areas. Mucous membranes, such as the mouth, are also typically involved. Complications include dehydration, sepsis, pneumonia, and multiple organ failure.

Staphylococcal scalded skin syndrome (SSSS) is a dermatological condition caused by Staphylococcus aureus.

Glossitis can mean soreness of the tongue, or more usually inflammation with depapillation of the dorsal surface of the tongue, leaving a smooth and erythematous (reddened) surface,. In a wider sense, glossitis can mean inflammation of the tongue generally. Glossitis is often caused by nutritional deficiencies and may be painless or cause discomfort. Glossitis usually responds well to treatment if the cause is identified and corrected. Tongue soreness caused by glossitis is differentiated from burning mouth syndrome, where there is no identifiable change in the appearance of the tongue, and there are no identifiable causes.

Gingivostomatitis is a combination of gingivitis and stomatitis, or an inflammation of the oral mucosa and gingiva. Herpetic gingivostomatitis is often the initial presentation during the first ("primary") herpes simplex infection. It is of greater severity than herpes labialis which is often the subsequent presentations. Primary herpetic gingivostomatitis is the most common viral infection of the mouth.

Angular cheilitis (AC) is inflammation of one or both corners of the mouth. Often the corners are red with skin breakdown and crusting. It can also be itchy or painful. The condition can last for days to years. Angular cheilitis is a type of cheilitis.
A genital ulcer is an open sore located on the genital area, which includes the vulva, penis, perianal region, or anus. Genital ulcers are most commonly caused by infectious agents. However, this is not always the case, as a genital ulcer may have noninfectious causes as well.
Herpes gladiatorum is one of the most infectious of herpes-caused diseases, and is transmissible by skin-to-skin contact. The disease was first described in the 1960s in the New England Journal of Medicine. It is caused by contagious infection with human herpes simplex virus type 1 (HSV-1), which more commonly causes oral herpes. Another strain, HSV-2 usually causes genital herpes, although the strains are very similar and either can cause herpes in any location.

In medicine, a drug eruption is an adverse drug reaction of the skin. Most drug-induced cutaneous reactions are mild and disappear when the offending drug is withdrawn. These are called "simple" drug eruptions. However, more serious drug eruptions may be associated with organ injury such as liver or kidney damage and are categorized as "complex". Drugs can also cause hair and nail changes, affect the mucous membranes, or cause itching without outward skin changes.
Paraneoplastic pemphigus (PNP) is an autoimmune disorder stemming from an underlying tumor. It is hypothesized that antigens associated with the tumor trigger an immune response resulting in blistering of the skin and mucous membranes.
Id reactions are types of acute dermatitis developing after days or weeks at skin locations distant from the initial inflammatory or infectious site. They can be localised or generalised. This is also known as an 'autoeczematous response' and there must be an identifiable initial inflammatory or infectious skin problem which leads to the generalised eczema. Often intensely itchy, the red papules and pustules can also be associated with blisters and scales and are always remote from the primary lesion. It is most commonly a blistering rash with itchy vesicles on the sides of fingers and feet as a reaction to fungal infection on the feet, athlete's foot. Stasis dermatitis, allergic contact dermatitis, acute irritant contact eczema and infective dermatitis have been documented as possible triggers, but the exact cause and mechanism is not fully understood. Several other types of id reactions exist including erythema nodosum, erythema multiforme, Sweet's syndrome and urticaria.
Bullous drug reaction most commonly refers to a drug reaction in the erythema multiforme group. These are uncommon reactions to medications, with an incidence of 0.4 to 1.2 per million person-years for toxic epidermal necrolysis and 1.2 to 6.0 per million person-years for Stevens–Johnson syndrome. The primary skin lesions are large erythemas, most often irregularly distributed and of a characteristic purplish-livid color, at times with flaccid blisters.
Erythema multiforme is usually a reaction of the skin and mucous membranes that occurs suddenly. It appears as a symmetrical rash and may include the mucous membrane lesions. This means that the body is sensitive to something that causes the skin and mucous membranes to react. The more common mild form is refer to as EM minor. It consists of a skin rash that involve no more than one mucosal surface. The sudden onset will progress rapidly as symmetrical lesions with circular color changes in some or all of the lesions. Rash will spread towards center or trunk of the body. Evenly distributed bumps on the skin become classic iris or target lesions. They have bright red borders and small white bumps in the center. The cause of EM appears to be a highly sensitive reaction that can be triggered by a variety of causes. The causes can include bacterial, viral or chemical products, such as antibiotics – specifically penicillins or cephalosporins. This reaction is an allergic reaction and is in no way contagious.
Erythema multiforme major is a form of rash with skin loss or epidermal detachment.

A cold sore is a type of herpes infection caused by the herpes simplex virus that affects primarily the lip. Symptoms typically include a burning pain followed by small blisters or sores. The first attack may also be accompanied by fever, sore throat, and enlarged lymph nodes. The rash usually heals within ten days, but the virus remains dormant in the trigeminal ganglion. The virus may periodically reactivate to create another outbreak of sores in the mouth or lip.
In dermatology, a target lesion or bull's-eye lesion, named for its resemblance to the bull's-eye of a shooting target, is a rash with central clearing. It occurs in several diseases, as follows:
A vulvar disease is a particular abnormal, pathological condition that affects part or all of the vulva. Several pathologies are defined. Some can be prevented by vulvovaginal health maintenance.
 Target lesion
Target lesion Erythema Multiforme target lesions on the leg
Erythema Multiforme target lesions on the leg


